

The cox-maze procedure for lone atrial fibrillation: a single-center experience over 2 decades
- PMID: 22095640
- PMCID: PMC3288520
- DOI: 10.1161/CIRCEP.111.963819
The cox-maze procedure for lone atrial fibrillation: a single-center experience over 2 decades
Abstract
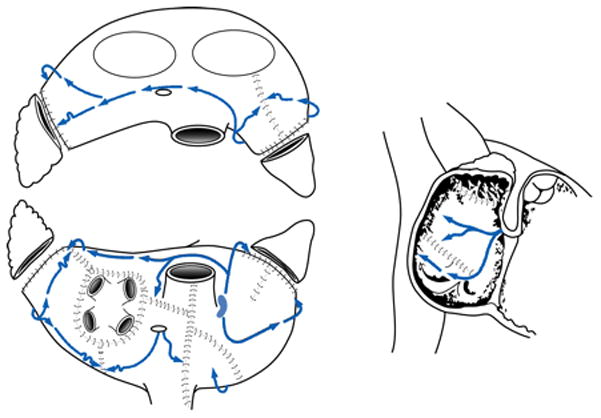
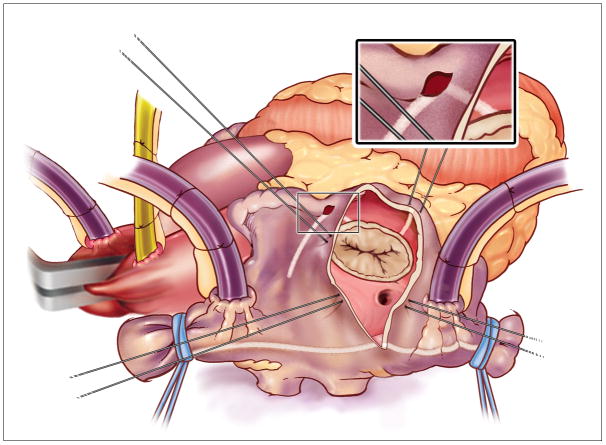
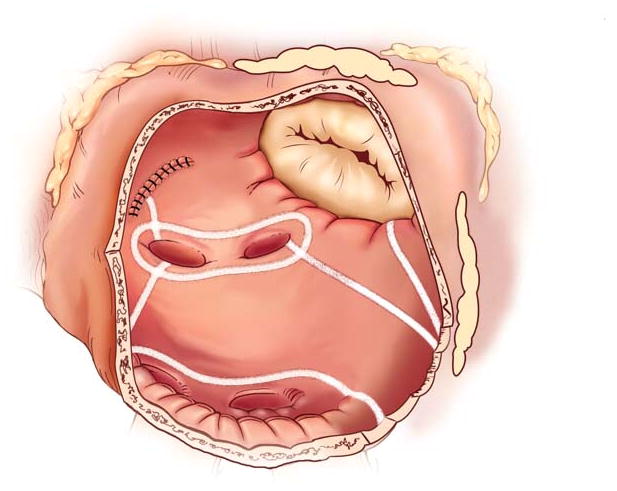
Background: The Cox-Maze procedure (CMP) has achieved high success rates in the therapy of atrial fibrillation (AF) while becoming progressively less invasive. This report evaluates our experience with the CMP in the treatment of lone AF over 2 decades and compares the original cut-and-sew CMP-III to the ablation-assisted CMP-IV, which uses bipolar radiofrequency and cryoenergy to create the original lesion pattern.
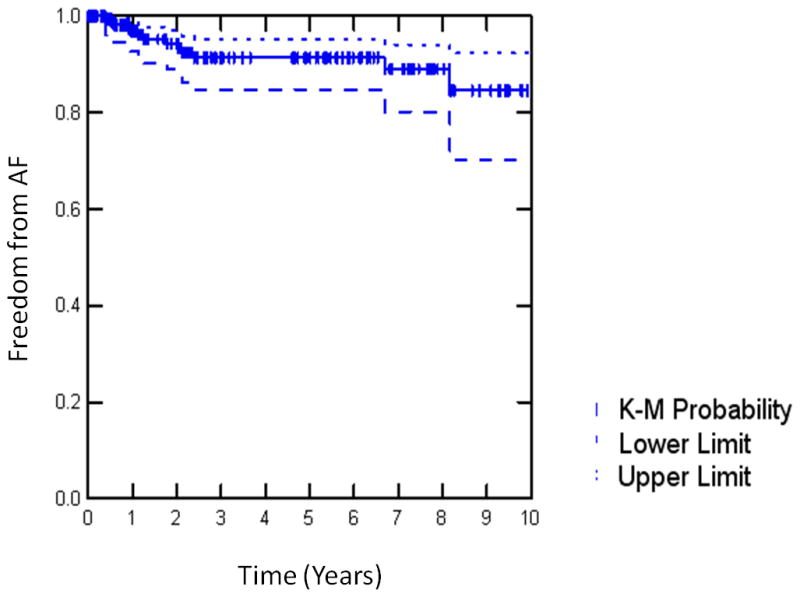
Methods and results: Data were collected prospectively on 212 consecutive patients (mean age, 53.5±10.4 years; 78% male) who underwent a stand-alone CMP from 1992 through 2010. The median duration of preoperative AF was 6 (interquartile range, 2.9-11.5) years, with 48% paroxysmal and 52% persistent or long-standing persistent AF. Univariate analysis with preoperative and perioperative variables used as covariates for the CMP-III (n=112) and the CMP-IV (n=100) was performed. Overall, 30-day mortality was 1.4%, with no intraoperative deaths. Freedom from AF was 93%, and freedom from AF off antiarrhythmics was 82%, at a mean follow-up time of 3.6±3.1 years. Freedom from symptomatic AF at 10 years was 85%. Only 1 late stroke occurred, with 80% of patients not receiving anticoagulation therapy. The less invasive CMP-IV had significantly shorter cross-clamp times (41±13 versus 92±26 minutes; P<0.001) while achieving high success rates, with 90% freedom from AF and 84% freedom from AF off antiarrhythmics at 2 years.
Conclusions: The CMP, although simplified and shortened by alternative energy sources, has excellent results, even with improved follow-up and stricter definition of failure.
Conflict of interest statement
Figures
References
-
- Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS, D'Agostino RB, Massaro JM, Beiser A, Wolf PA, Benjamin EJ. Lifetime risk for development of atrial fibrillation: The framingham heart study. Circulation. 2004;110:1042–1046. - PubMed
-
- Thom T, Haase N, Rosamond W, Howard VJ, Rumsfeld J, Manolio T, Zheng ZJ, Flegal K, O'Donnell C, Kittner S, Lloyd-Jones D, Goff DC, Jr, Hong Y, Adams R, Friday G, Furie K, Gorelick P, Kissela B, Marler J, Meigs J, Roger V, Sidney S, Sorlie P, Steinberger J, Wasserthiel-Smoller S, Wilson M, Wolf P. Heart disease and stroke statistics--2006 update: A report from the american heart association statistics committee and stroke statistics subcommittee. Circulation. 2006;113:e85–151. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: The framingham study. Stroke. 1991;22:983–988. - PubMed
-
- Marcus GM, Sung RJ. Antiarrhythmic agents in facilitating electrical cardioversion of atrial fibrillation and promoting maintenance of sinus rhythm. Cardiology. 2001;95:1–8. - PubMed
-
- Wann LS, Curtis AB, January CT, Ellenbogen KA, Lowe JE, Estes NA, 3rd, Page RL, Ezekowitz MD, Slotwiner DJ, Jackman WM, Stevenson WG, Tracy CM, Fuster V, Ryden LE, Cannom DS, Le Heuzey JY, Crijns HJ, Olsson SB, Prystowsky EN, Halperin JL, Tamargo JL, Kay GN, Jacobs AK, Anderson JL, Albert N, Hochman JS, Buller CE, Kushner FG, Creager MA, Ohman EM, Ettinger SM, Guyton RA, Tarkington LG, Yancy CW. 2011 accf/aha/hrs focused update on the management of patients with atrial fibrillation (updating the 2006 guideline): A report of the american college of cardiology foundation/american heart association task force on practice guidelines. Circulation. 2011;123:104–123.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
