

Circadian dependence of infarct size and left ventricular function after ST elevation myocardial infarction
- PMID: 22095727
- PMCID: PMC3253266
- DOI: 10.1161/CIRCRESAHA.111.254284
Circadian dependence of infarct size and left ventricular function after ST elevation myocardial infarction
Abstract
Rationale: In rodents, infarct size after ischemia/reperfusion exhibits a circadian dependence on the time of coronary occlusion. It is not known if a similar circadian dependence of infarct size occurs in humans.
Objective: To determine if humans exhibit a circadian dependence of infarct size in the setting of ST elevation myocardial infarction (STEMI).
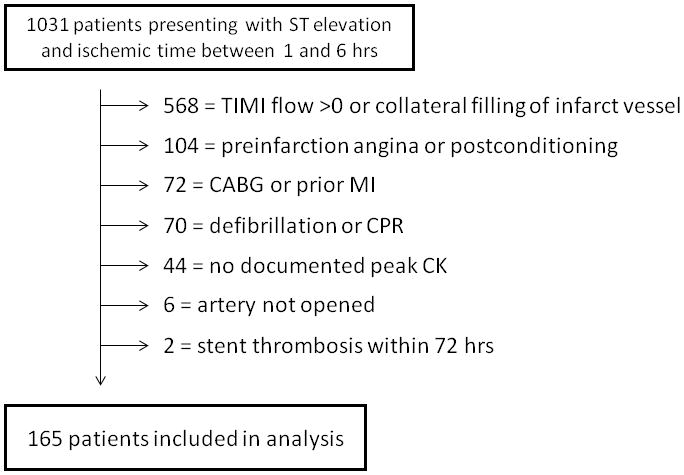
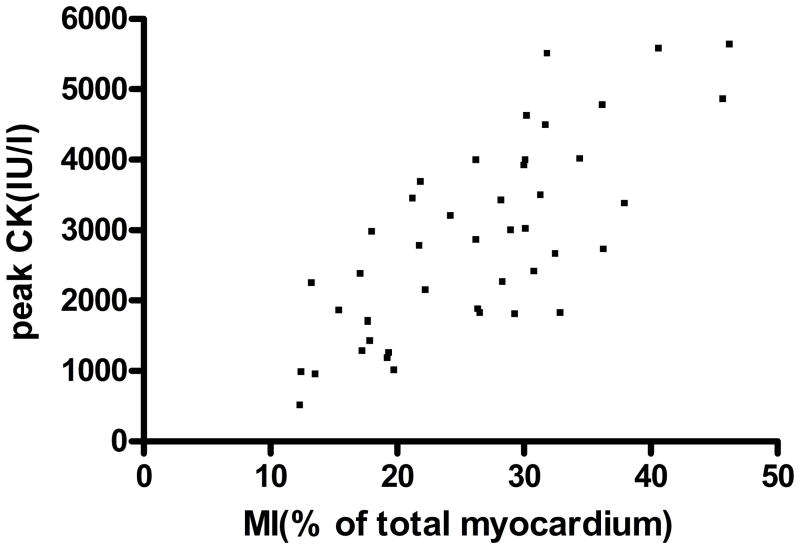
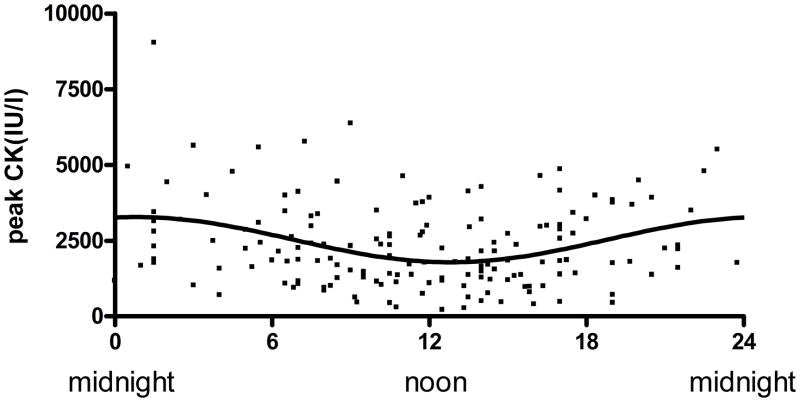
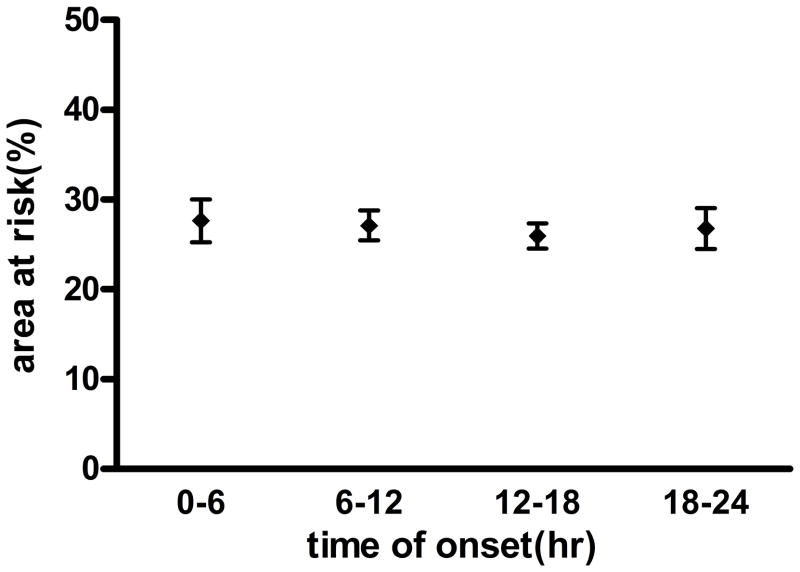
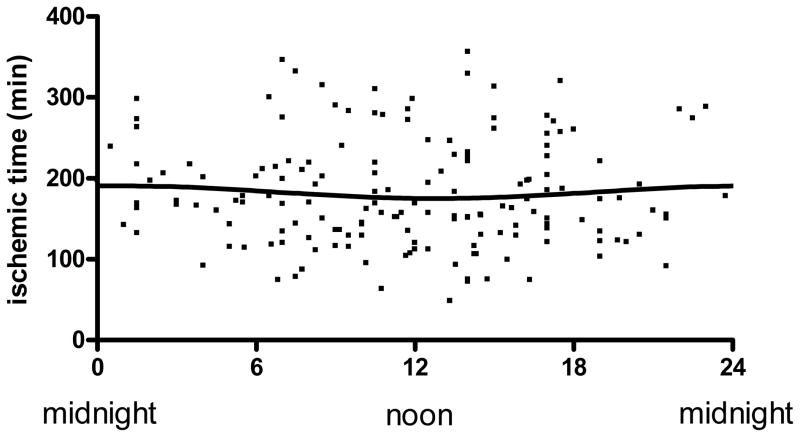
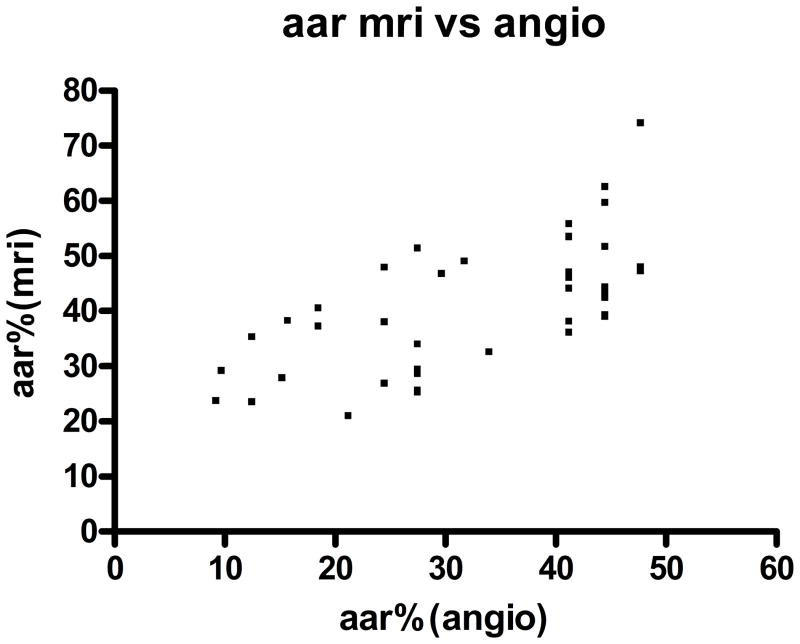
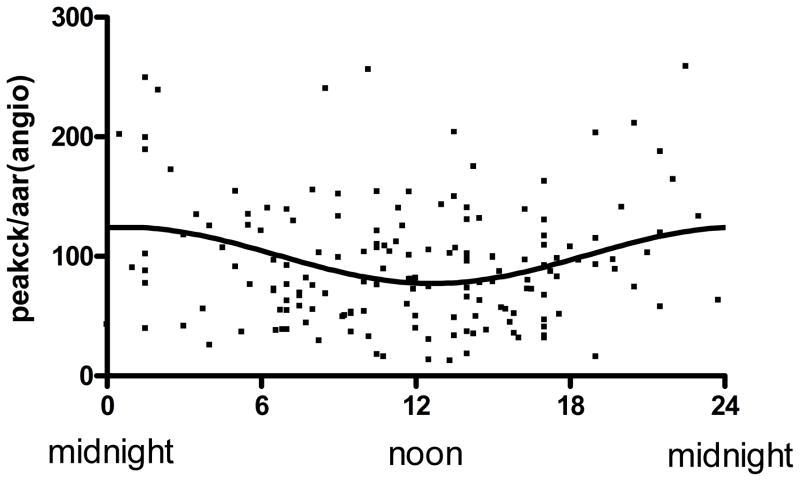
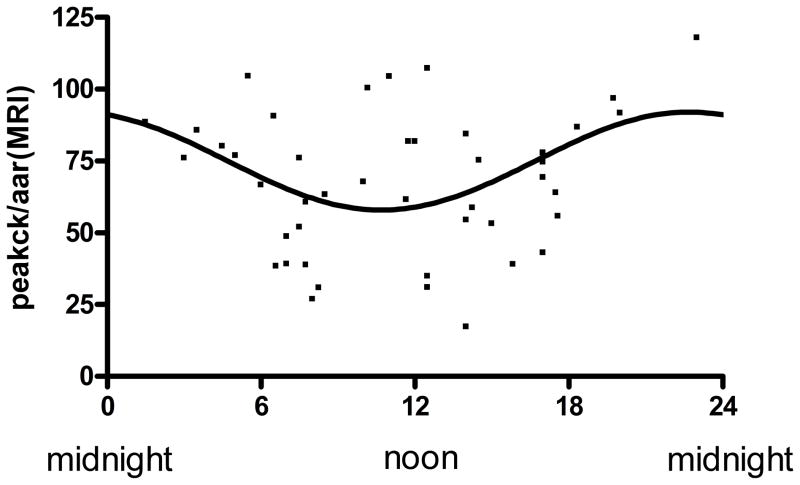
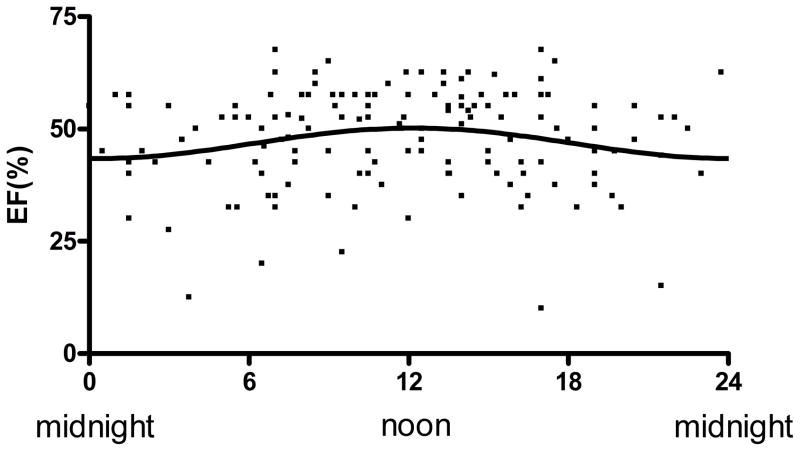
Methods and results: A retrospective analysis of 1031 patients with STEMI referred for primary percutaneous coronary intervention with known ischemic times between 1 and 6 hours identified 165 patients with occluded arteries on presentation without evidence of preinfarction angina or collateral blood flow. Both ischemic duration and angiographic area at risk were not dependent on time of infarct onset. We observed that the extent of infarct size measured by creatine kinase release was significantly associated with time of day onset of infarction (P<0.0001). The greatest myocardial injury occurred at 1:00 am onset of ischemia and 5:00 am onset of reperfusion, with the peak creatine kinase measured at the peak of the curve being 82% higher than that recorded at the trough. Similarly, left ventricular ejection fraction measured within 2 days of infarction was also dependent on time of onset of STEMI with the absolute left ventricular ejection fraction at peak >7% higher than at trough (43% vs 51%; P<0.03). These findings were supported by a subgroup of patients (n = 45) who underwent cardiac MRI measurements of infarct size and area-at-risk measurements.
Conclusions: The results of this study demonstrate for the first time in humans that myocardial infarct size and left ventricular function after STEMI have a circadian dependence on the time of day onset of ischemia.
Figures
Comment in
-
On circadian variation of myocardial reperfusion injury.Circ Res. 2012 Jan 6;110(1):6-7. doi: 10.1161/CIRCRESAHA.111.260265. Circ Res. 2012. PMID: 22223205 No abstract available.
-
Circadian variations of infarct size in STEM1.Circ Res. 2012 Feb 3;110(3):e22; author reply e23. doi: 10.1161/CIRCRESAHA.111.262816. Circ Res. 2012. PMID: 22302758 No abstract available.
-
Finding the real culprit between circadian rhythm and "out of hours effect" to explain the higher myocardial infarction size among patients with symptom onset occurring at night.Circ Res. 2012 Apr 27;110(9):e67; author reply e68. doi: 10.1161/CIRCRESAHA.112.269076. Circ Res. 2012. PMID: 22539760 No abstract available.
-
Questing for circadian dependence in ST-segment-elevation acute myocardial infarction: a multicentric and multiethnic study.Circ Res. 2013 May 10;112(10):e110-4. doi: 10.1161/CIRCRESAHA.112.300778. Circ Res. 2013. PMID: 23661713
-
Of mice and men: the quest to determine a circadian basis for myocardial protection in ischemia/reperfusion injury.Circ Res. 2013 May 10;112(10):e115-7. doi: 10.1161/CIRCRESAHA.113.301079. Circ Res. 2013. PMID: 23661714 No abstract available.
-
Still need for compelling evidence to support the circadian dependence of infarct size after ST-elevation myocardial infarction.Circ Res. 2013 Aug 2;113(4):e43-4. doi: 10.1161/CIRCRESAHA.113.301908. Circ Res. 2013. PMID: 23908336 No abstract available.
References
-
- Muller JE, Tofler GH, Stone PH. Circadian variation and triggers of onset of acute cardiovascular disease. Circulation. 1989;79:733–743. - PubMed
-
- Nomura S, Fujitaka M, Sakura N, Ueda K. Circadian rhythms in plasma cortisone and cortisol and the cortisone/cortisol ratio. Clinica Chimica Acta. 1997;266:83–91. - PubMed
-
- Muller JE, Stone PH, Turi ZG, et al. Circadian variation in the frequency of onset of acute myocardial infarction. N Engl J Med. 1985;313:1315–22. - PubMed
-
- Muller JE, Ludmer PL, Willich SN, Tofler GH, Aylmer G, Kangos I. Circadian variation in the frequency of sudden cardiac death. Circulation. 1987;75:131–38. - PubMed
-
- Mahmoud KD, Lennon RJ, Ting HH, Rihal CS, Holmes DR. Circadian variation in coronary stent thrombosis. J Am Coll Cardiol Intv. 2011;4:183–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
