

Reperfusion by combined thrombolysis and mechanical thrombectomy in acute stroke: effect of collateralization, mismatch, and time to and grade of recanalization on clinical and tissue outcome
- PMID: 22095969
- PMCID: PMC7964811
- DOI: 10.3174/ajnr.A2746
Reperfusion by combined thrombolysis and mechanical thrombectomy in acute stroke: effect of collateralization, mismatch, and time to and grade of recanalization on clinical and tissue outcome
Abstract
Background and purpose: Our research focuses on interventional neuroradiology (stroke treatment including imaging methods) and general neuroimaging with an emphasis on functional MR imaging. Our aim was to determine the efficacy of revascularization (TIMI) of middle cerebral and/or carotid artery occlusion by means of mechanical recanalization techniques and to evaluate the impact of collateralization, mismatch in perfusion CT, time to revascularization, grade of revascularization on tissue, and clinical outcome in patients with acute ischemic stroke.
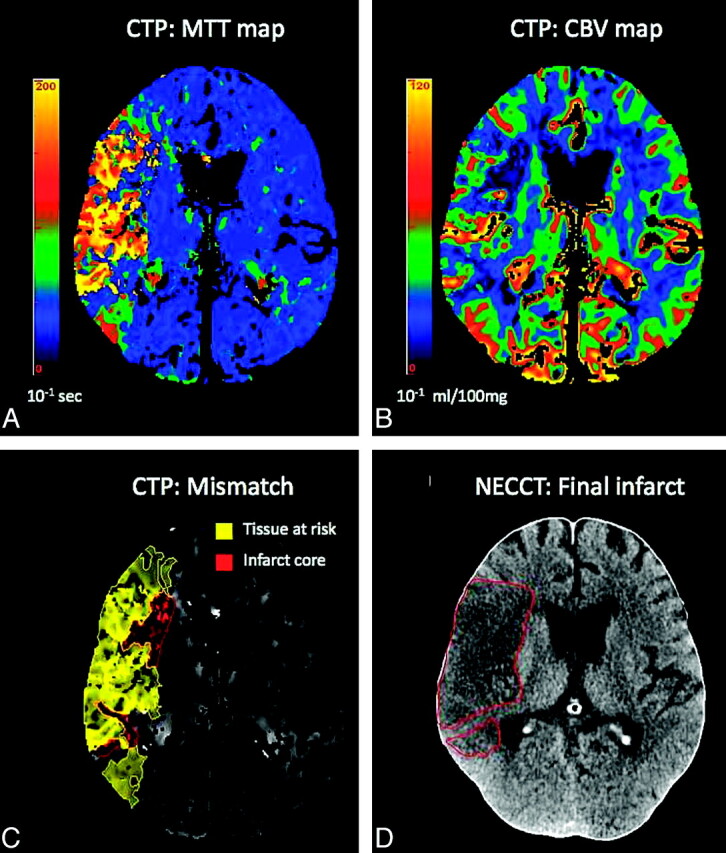
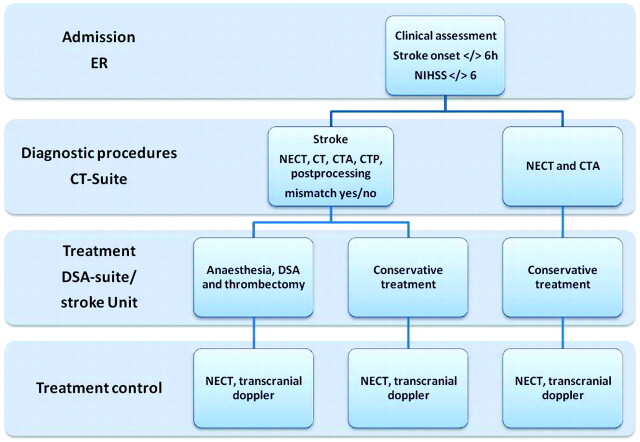
Materials and methods: Thirty-one patients with MCA and/or ICA occlusion were included. Ischemic stroke was diagnosed by NECT, CTA, and volume PCT for grading collateralization and mismatch. Time to recanalization was measured from the onset of stroke to the time point of DSA-proved mechanical recanalization. Tissue outcome was calculated by segmentation of infarct size between pre- and postinterventional CT and percentage mismatch lost. Clinical outcome was determined by the mRS.
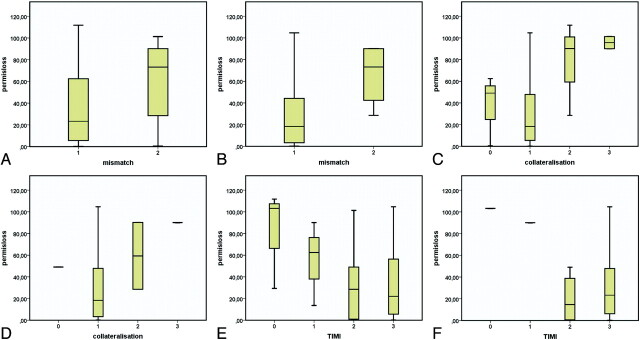
Results: Twenty-one of 31 patients (61.8%) presented with MCA and 10/31 patients (38.2%), with distal ICA occlusions. Sufficient recanalization (TIMI 2 and 3) was achieved in 23/31 (75%). Clinical evaluation revealed an mRS score of ≤2 in 25.5%. Age (r = 0.439, P = .038) and TIMI (r = 0.544, P = .002) showed the strongest correlation with clinical outcome. Time to recanalization, TIMI score, and mismatch were associated with a good tissue outcome in ANOVA.
Conclusions: Favorable outcome after mechanical recanalization of acute MCA and ICA occlusion depends on time to and grade of recanalization, mismatch, and collateralization. These results indicate that multimodal stroke imaging is helpful to guide therapy decisions and to indicate patients amenable for mechanical recanalization.
Figures
References
-
- Struffert T, Kohrmann M, Engelhorn T, et al. . Penumbra stroke system as an “add-on” for the treatment of large vessel occlusive disease following thrombolysis: first results. Eur Radiol 2009; 19: 2286– 93 - PubMed
-
- Liebig T LJ, Reinartz J, Roth C, et al. . Early clinical experiences with new thrombectomy device for the treatment of ischemic stroke. In: Proceedings of the International Stroke Conference, New Orleans, Louisiana. February 20–22, 2008
-
- Flint AC, Duckwiler GR, Budzik RF, et al. . Mechanical thrombectomy of intracranial internal carotid occlusion: pooled results of the MERCI and Multi MERCI Part I trials. Stroke 2007; 38: 1274– 80. Epub 2007 Mar 1 - PubMed
-
- Castano C, Dorado L, Guerrero C, et al. . Comment on: Mechanical thrombectomy with the Solitaire AB device in large artery occlusions of the anterior circulation: Castaño C, Dorado L, Guerrero C, et al. Stroke 2010;41:1836–40. Clin Neuroradiol 2010; 20: 267– 68. Epub 2010 Dec 3 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous