

IL-2 stimulated but not unstimulated NK cells induce selective disappearance of peripheral blood cells: concomitant results to a phase I/II study
- PMID: 22096557
- PMCID: PMC3212563
- DOI: 10.1371/journal.pone.0027351
IL-2 stimulated but not unstimulated NK cells induce selective disappearance of peripheral blood cells: concomitant results to a phase I/II study
Abstract
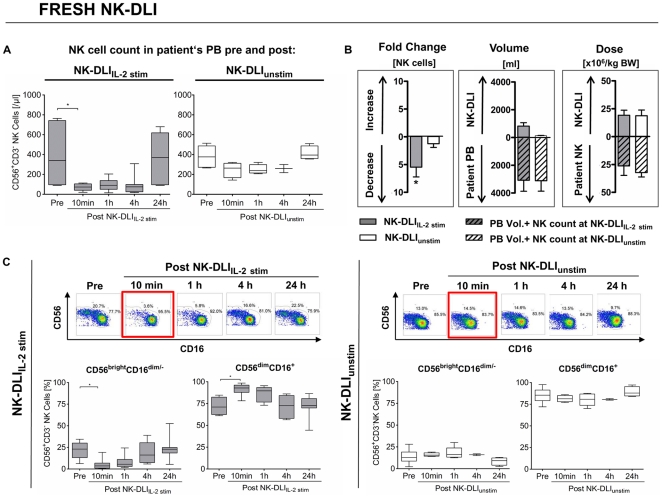
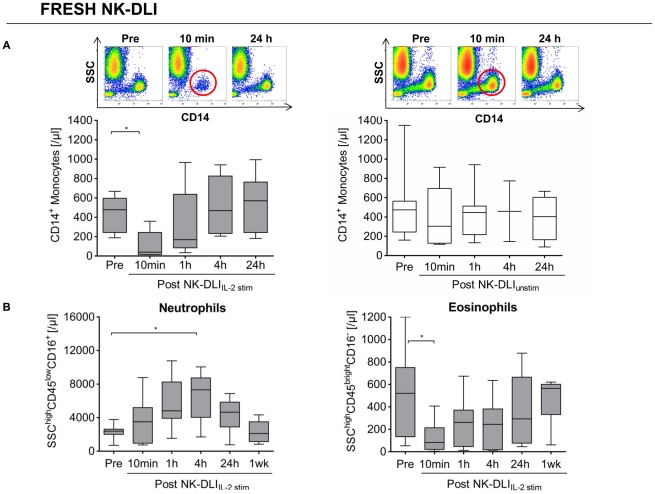
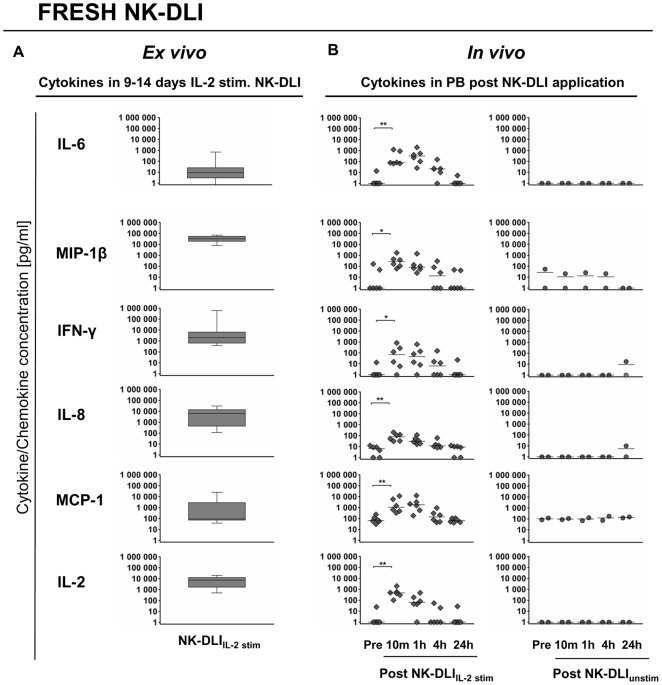
In an ongoing clinical phase I/II study, 16 pediatric patients suffering from high risk leukemia/tumors received highly purified donor natural killer (NK) cell immunotherapy (NK-DLI) at day (+3) +40 and +100 post haploidentical stem cell transplantation. However, literature about the influence of NK-DLI on recipient's immune system is scarce. Here we present concomitant results of a noninvasive in vivo monitoring approach of recipient's peripheral blood (PB) cells after transfer of either unstimulated (NK-DLI(unstim)) or IL-2 (1000 U/ml, 9-14 days) activated NK cells (NK-DLI(IL-2 stim)) along with their ex vivo secreted cytokine/chemokines. We performed phenotypical and functional characterizations of the NK-DLIs, detailed flow cytometric analyses of various PB cells and comprehensive cytokine/chemokine arrays before and after NK-DLI. Patients of both groups were comparable with regard to remission status, immune reconstitution, donor chimerism, KIR mismatching, stem cell and NK-DLI dose. Only after NK-DLI(IL-2 stim) was a rapid, almost complete loss of CD56(bright)CD16(dim/-) immune regulatory and CD56(dim)CD16(+) cytotoxic NK cells, monocytes, dendritic cells and eosinophils from PB circulation seen 10 min after infusion, while neutrophils significantly increased. The reduction of NK cells was due to both, a decrease in patients' own CD69(-) NCR(low)CD62L(+) NK cells as well as to a diminishing of the transferred cells from the NK-DLI(IL-2 stim) with the CD56(bright)CD16(+/-)CD69(+)NCR(high)CD62L(-) phenotype. All cell counts recovered within the next 24 h. Transfer of NK-DLI(IL-2 stim) translated into significantly increased levels of various cytokines/chemokines (i.e. IFN-γ, IL-6, MIP-1β) in patients' PB. Those remained stable for at least 1 h, presumably leading to endothelial activation, leukocyte adhesion and/or extravasation. In contrast, NK-DLI(unstim) did not cause any of the observed effects. In conclusion, we assume that the adoptive transfer of NK-DLI(IL-2 stim) under the influence of ex vivo and in vivo secreted cytokines/chemokines may promote NK cell trafficking and therefore might enhance efficacy of immunotherapy.
Conflict of interest statement
Figures
References
-
- Passweg JR, Koehl U, Uharek L, Meyer-Monard S, Tichelli A. Natural-killer-cell-based treatment in haematopoietic stem-cell transplantation. Best Pract Res Clin Haematol. 2006;19:811–824. - PubMed
-
- Passweg JR, Stern M, Koehl U, Uharek L, Tichelli A. Use of natural killer cells in hematopoetic stem cell transplantation. Bone Marrow Transplant. 2005;35:637–643. - PubMed
-
- Lanier LL. NK cell recognition. Annu Rev Immunol. 2005;23:225–274. - PubMed
-
- Moretta A, Bottino C, Vitale M, Pende D, Cantoni C, et al. Activating receptors and coreceptors involved in human natural killer cell-mediated cytolysis. Annu Rev Immunol. 2001;19:197–223. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
