

CONTINUOUS REPOPULATION OF LYMPHOCYTE SUBSETS IN TRANSPLANTED MYCOBACTERIAL GRANULOMAS
- PMID: 22096617
- PMCID: PMC3215294
- DOI: 10.1556/EuJMI.1.2011.1.8
CONTINUOUS REPOPULATION OF LYMPHOCYTE SUBSETS IN TRANSPLANTED MYCOBACTERIAL GRANULOMAS
Abstract
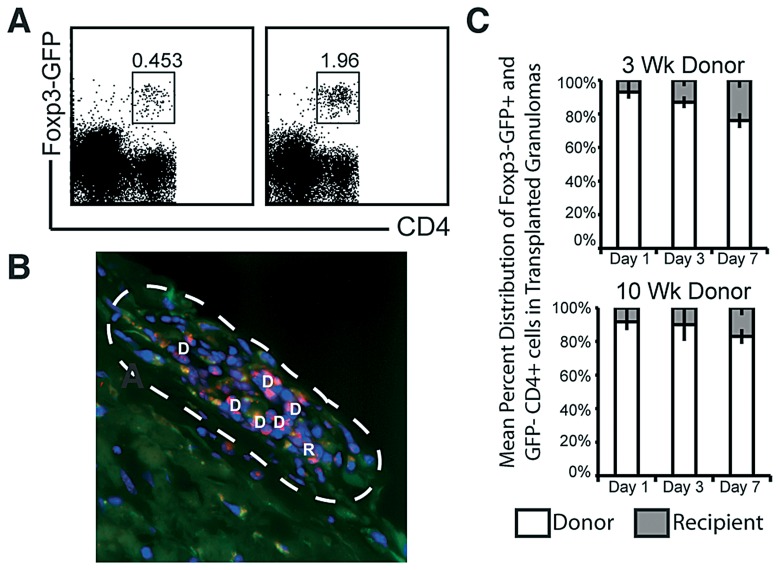
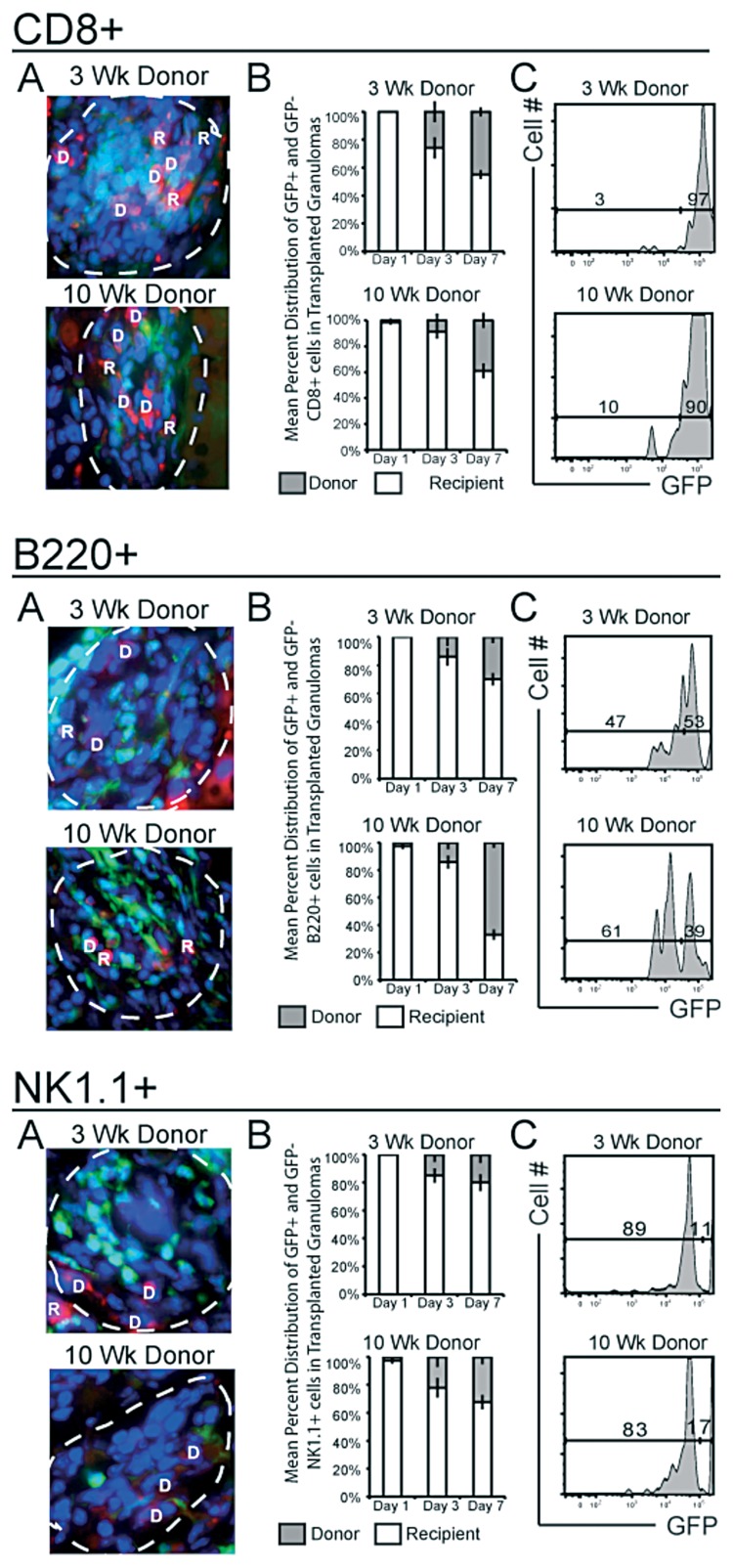
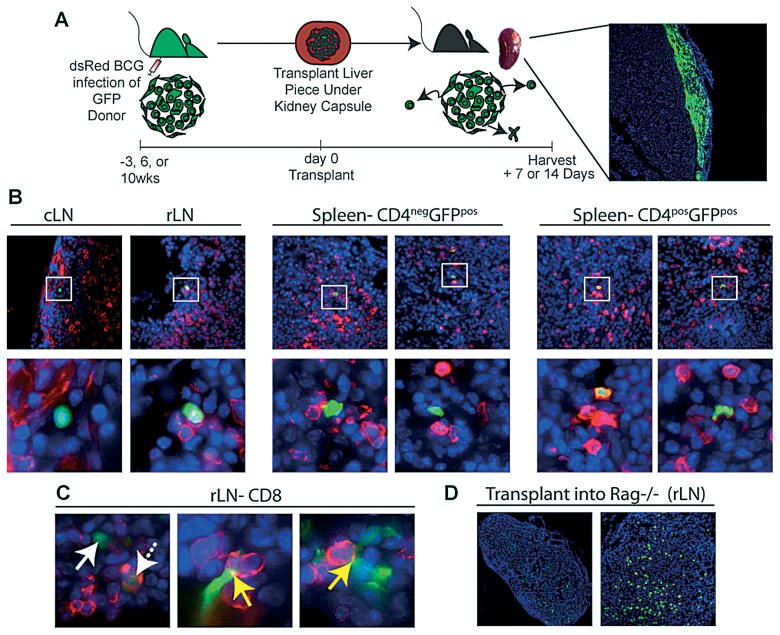
Granulomas are the interface between host and mycobacteria, and are crucial for the surivival of both species. While macrophages are the main cellular component of these lesions, different lymphocyte subpopulations within the lesions also play important roles. Lymphocytes are continuously recruited into these inflammatory lesions via local vessels to replace cells that are either dying or leaving; however, their rate of replacement is not known. Using a model of granuloma transplantation and fluorescently labeled cellular compartments we report that, depending on the subpopulation, 10-80%, of cells in the granuloma are replaced within one week after transplantation. CD4(+) T cells specific for Mycobacterium antigen entered transplanted granulomas at a higher frequency than Foxp3(+) CD4(+) T cells by one week. Interestingly, a small number of T lymphocytes migrated out of the granuloma to secondary lymphoid organs. The mechanisms that define the differences in recruitment and efflux behind each subpopulation requires further studies. Ultimately, a better understanding of lymphoid traffic may provide new ways to modulate, regulate, and treat granulomatous diseases.
Figures
References
-
- Ulrichs T, Kaufmann SH. New insights into the function of granulomas in human tuberculosis. J Pathol. 2006 Jan;208(2):261–269. - PubMed
-
- Co DO, Hogan LH, Kim SI, Sandor M. Mycobacterial granulomas: keys to a long-lasting host-pathogen relationship. Clin Immunol. 2004 Nov;113(2):130–136. - PubMed
-
- Schreiber HA, Hulseberg PD, Lee J, Prechl J, Barta P, Szlavik N, Harding JS, Fabry Z, Sandor M. Dendritic cells in chronic mycobacterial granulomas restrict local anti-bacterial T cell response in a murine model. PLoS One. 2010 Jul 6;5(7):e11453. doi: 10.1371/journal.pone.0011453. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials