

Guided growth for ankle valgus
- PMID: 22101668
- PMCID: PMC3227545
- DOI: 10.1097/BPO.0b013e318236b1df
Guided growth for ankle valgus
Abstract
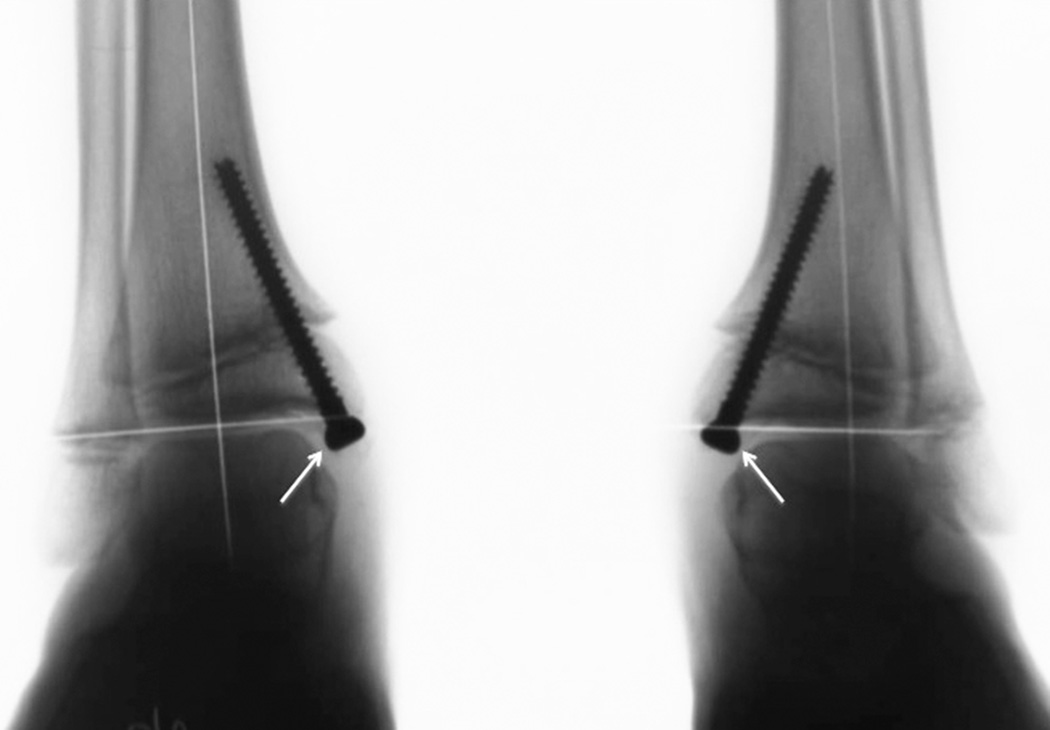
Background: Ankle valgus may be insidious and common in a variety of congenital conditions including clubfoot, neuromuscular disorders and others or acquired after fracture, osteotomies, or other manipulations of the lower extremity. This can cause hindfoot pronaton, resulting in lateral impingement and excessive shoe wear. Orthoses do not change the natural history. Medial hemiepiphysiodesis of the tibia is an accepted method of correcting this problem. Difficulties with transmalleolor screw removal prompted us to adopt the tension band method. Our purpose was to outline the technique of using guided growth with a medial tension band plate and discuss the efficacy of this technique.
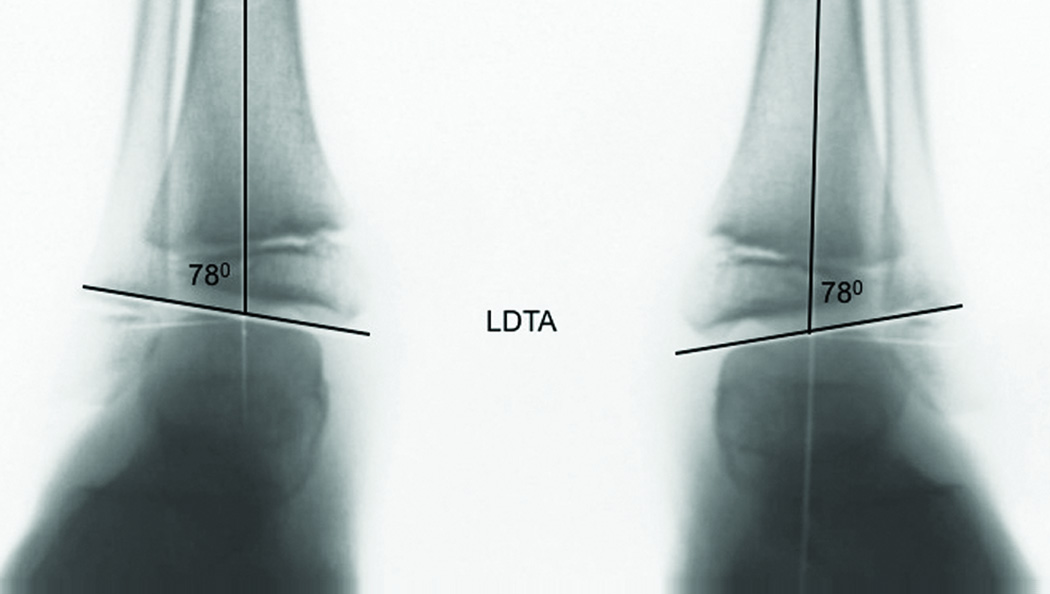
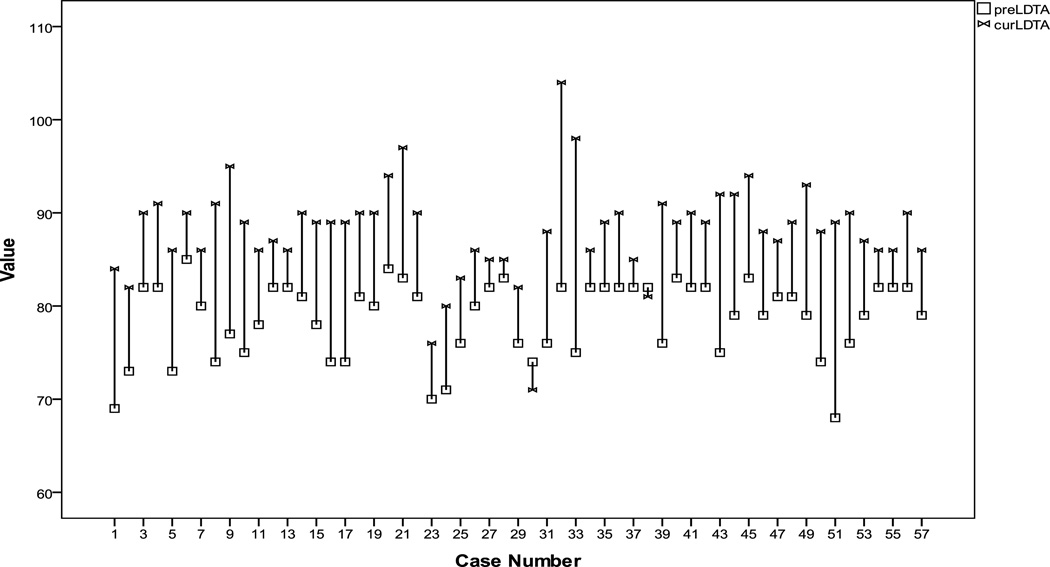
Methods: We undertook this retrospective review of 33 patients (57 ankles) who underwent guided growth to correct ankle valgus and were followed until attaining full correction or skeletal maturity. Most of the implants were removed when the ankle was neutral to 5 degrees of varus overcorrection. We obtained weightbearing anteroposterior radiographs of the ankles preoperatively, just before plate removal, and at final follow-up, measuring the lateral distal tibial angle and noting the fibular station. We documented the rate of correction and related complications.
Results: The average age at surgery was 10.4 years (range, 6.1 to 14.6 y) and an average follow-up was 27 months (range, 12 to 57.5 mo). The lateral distal tibial angle improved from an average of 78.7 to 90 degrees at implant removal and measured 88.2 degrees at final follow-up. The rate of correction was calculated to be 0.6 degrees per month. The fibular station remained the same in 36 of 57 ankles and improved in 15 ankles. There were 2 cases of skin breakdown complicated by infection. There were no instances of hardware failure, excessive varus, or premature physeal closure and no patient has required an osteotomy.
Conclusions: Without appropriate radiographs, ankle valgus may be mistaken for hindfoot valgus and mismanaged accordingly. Guided growth of the distal medial tibia has become our treatment of choice for ankle valgus in the growing child or adolescent. Use of plate epiphysiodesis is safe, well tolerated, may readily be combined with other treatments, and provides a rate of correction comparable to the transmalleolar screw method.
Level of evidence: IV, retrospective review, no control series.
Figures



Similar articles
-
Medial malleolar screw versus tension-band plate hemiepiphysiodesis for ankle valgus in the skeletally immature.J Pediatr Orthop. 2014 Jun;34(4):441-6. doi: 10.1097/BPO.0000000000000116. J Pediatr Orthop. 2014. PMID: 24172668
-
Ankle valgus and clubfeet.J Pediatr Orthop. 1999 Jul-Aug;19(4):515-7. doi: 10.1097/00004694-199907000-00018. J Pediatr Orthop. 1999. PMID: 10413004
-
Rate of Correction and Recurrence of Ankle Valgus in Children Using a Transphyseal Medial Malleolar Screw.J Pediatr Orthop. 2015 Sep;35(6):589-92. doi: 10.1097/BPO.0000000000000333. J Pediatr Orthop. 2015. PMID: 26251960
-
Progressive valgus angulation of the ankle secondary to loss of fibular congruity treated with medial tibial hemiepiphysiodesis and fibular reconstruction.Am J Orthop (Belle Mead NJ). 2014 Jun;43(6):280-3. Am J Orthop (Belle Mead NJ). 2014. PMID: 24945479 Review.
-
The indications and technique of supramalleolar osteotomy.Foot Ankle Clin. 2009 Sep;14(3):549-61. doi: 10.1016/j.fcl.2009.06.002. Foot Ankle Clin. 2009. PMID: 19712889 Review.
Cited by
-
Deformity progression in congenital posteromedial bowing of the tibia: a report of 44 cases.BMC Musculoskelet Disord. 2020 Jul 3;21(1):430. doi: 10.1186/s12891-020-03408-w. BMC Musculoskelet Disord. 2020. PMID: 32620101 Free PMC article.
-
Anterior Hemiepiphysiodesis of the Distal Tibia: A Step-by-step Surgical Technique Guide.Strategies Trauma Limb Reconstr. 2023 Sep-Dec;18(3):174-180. doi: 10.5005/jp-journals-10080-1596. Strategies Trauma Limb Reconstr. 2023. PMID: 38404566 Free PMC article.
-
Correction of ankle valgus by hemiepiphysiodesis using the tension band principle in patients with multiple hereditary exostosis.J Child Orthop. 2016 Jun;10(3):267-73. doi: 10.1007/s11832-016-0742-8. Epub 2016 May 27. J Child Orthop. 2016. PMID: 27234571 Free PMC article.
-
Risk factors for ankle valgus in children with hereditary multiple exostoses: a retrospective cross-sectional study.J Child Orthop. 2021 Aug 20;15(4):372-377. doi: 10.1302/1863-2548.15.210032. J Child Orthop. 2021. PMID: 34476027 Free PMC article.
-
Effective time, correction speed and termination time of hemi-epiphysiodesis in children.World J Orthop. 2024 Jan 18;15(1):1-10. doi: 10.5312/wjo.v15.i1.1. eCollection 2024 Jan 18. World J Orthop. 2024. PMID: 38293262 Free PMC article. Review.
References
-
- Malhotra D, Pau R, Owen R. Valgus Deformity of the Ankle in Children With Spina Bifida Aperta. J Bone Joint Surg. 1984;66:381–385. - PubMed
-
- Paley D, Herzenberg JE. Principles of Deformity Correction. Berlin Heidelberg New York: Springer-Verlag; 2002.
-
- Stevens PM, Otis S. Ankle Valgus and Clubfeet. J Pediatr Ortho. 1999;19:515–517. - PubMed
-
- Stevens PM, Arms D. Postaxial Hypoplasia of the Lower Extremity. J Peditr Ortho. 2000;20:166–172. - PubMed
-
- Noonan K, Feinberg, et al. Natural History of Multiple Hereditary Osteochondromatosis of the Lower Extremity and Ankle. J Pediatr Orthop. 2002;22:120–124. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
