

Too good to treat? Outcomes in patients not receiving thrombolysis due to mild deficits or rapidly improving symptoms
- PMID: 22103880
- PMCID: PMC3296877
- DOI: 10.1111/j.1747-4949.2011.00696.x
Too good to treat? Outcomes in patients not receiving thrombolysis due to mild deficits or rapidly improving symptoms
Abstract
Introduction: Among ischemic stroke patients arriving within the treatment window, rapidly improving symptoms or having a mild deficit (i.e. too good to treat) is a common reason for exclusion. Several studies have reported poor outcomes in this group. We addressed the question of early neurological deterioration in too good to treat patients in a larger prospective cohort study.
Methods: Admission and discharge information were collected prospectively in acute stroke patients who presented to the emergency room within three-hours from onset. The primary outcome measure was change in the National Institutes of Health Stroke Scale from baseline to discharge. Secondary outcomes were discharge National Institutes of Health Stroke Scale >4, not being discharged home, and discharge modified Rankin scale.
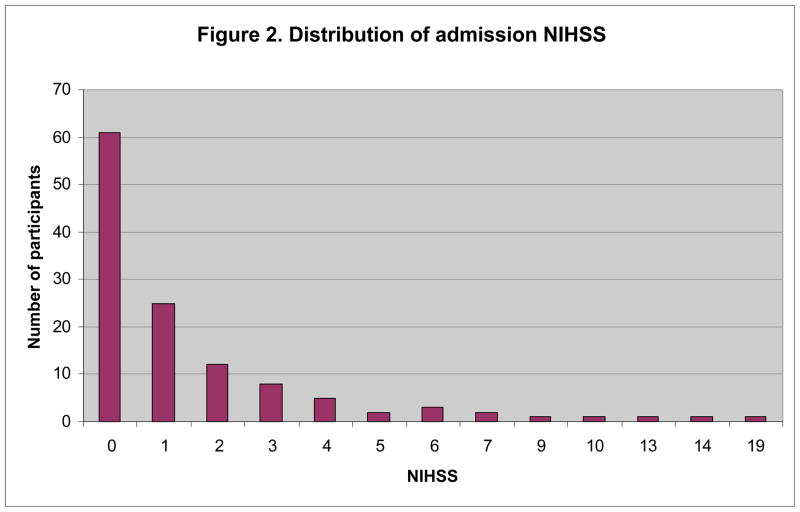
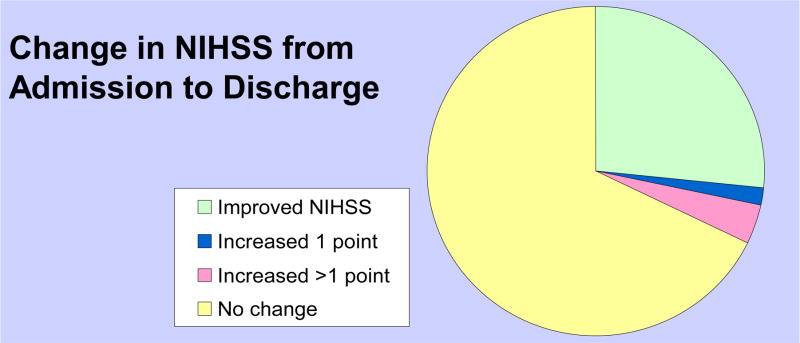
Results: Of 355 patients who presented within three-hours, 127 (35·8%) had too good to treat listed as the only reason for not receiving thrombolysis, with median admission National Institutes of Health Stroke Scale = 1 (range = 0 to 19). At discharge, seven (5·5%) showed a worsening of National Institutes of Health Stroke Scale ≥1, and nine (7·1%) had a National Institutes of Health Stroke Scale >4. When excluding prior stroke (remaining n = 97), discharge status was even more benign: only five (5·2%) had a discharge National Institutes of Health Stroke Scale >4, and two (2·1%) patients were not discharged home.
Conclusion: We found that a small proportion of patients deemed too good to treat will have early neurological deterioration, in contrast to other studies. Decisions about whether to treat mild stroke patients depend on the outcome measure chosen, particularly when considering discharge disposition among patients who have had prior stroke. The decision to thrombolyze may ultimately rest on the nature of the presentation and deficit.
© 2011 The Authors. International Journal of Stroke © 2011 World Stroke Organization.
Conflict of interest statement
Figures
References
-
- A systems approach to immediate evaluation and management of hyperacute stroke. Experience at eight centers and implications for community practice and patient care. The National Institute of Neurological Disorders and Stroke (NINDS) rt-PA Stroke Study Group. Stroke. 1997;28:1530–40. - PubMed
-
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. NEJM. 1995;333:1581–87. - PubMed
-
- Albers GW, Bates VE, Clark WM, Bell R, Verro P, Hamilton SA. Intravenous tissue-type plasminogen activator for treatment of acute stroke: the Standard Treatment with Alteplase to Reverse Stroke (STARS) study. JAMA. 2000;283:1145–50. - PubMed
-
- Tanne D, Bates VE, Verro P, et al. Initial clinical experience with IV tissue plasminogen activator for acute ischemic stroke: a multicenter survey. The t-PA Stroke SurveyGroup. Neurol. 1999;53:424–7. - PubMed
-
- Schumacher HC, Bateman BT, Boden-Albala B, et al. Use of thrombolysis in acute ischemic stroke: analysis of the Nationwide Inpatient Sample 1999 to 2004. AnnEmerg Med. 2007;50:99–107. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
