

Asthma in Head Start children: effects of the Breathmobile program and family communication on asthma outcomes
- PMID: 22104603
- PMCID: PMC3290717
- DOI: 10.1016/j.jaci.2011.10.013
Asthma in Head Start children: effects of the Breathmobile program and family communication on asthma outcomes
Abstract
Background: Asthma morbidity and mortality rates are high among young inner-city children. Lack of routine primary care provider visits, poor access to care, and poor patient-physician communication might be contributing factors.
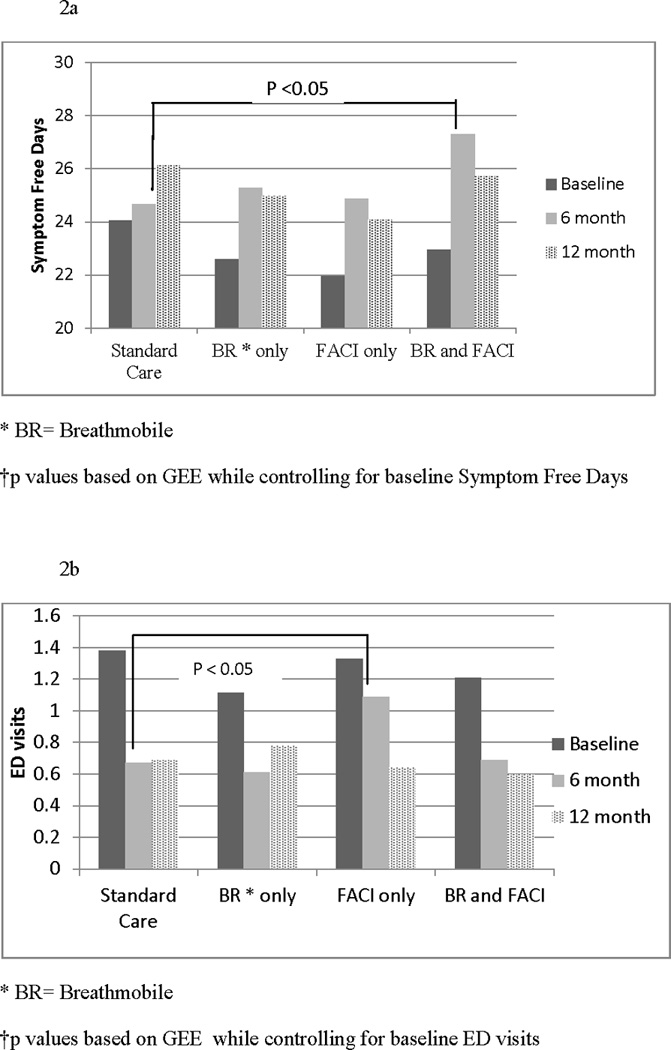
Objective: This study evaluated the effects of providing Breathmobile services only, a Facilitated Asthma Communication Intervention (FACI) only, or both Breathmobile plus FACI on asthma outcomes relative to standard care.
Methods: Children with asthma (n = 322; mean age, 4 years; 53% male; 97% African American) were recruited from Head Start programs in Baltimore City and randomized into 4 groups. Outcome measures included symptom-free days (SFDs), urgent care use (emergency department visits and hospitalizations), and medication use (courses of oral steroids and proportion taking an asthma controller medication), as reported by caregivers at baseline, 6-month, and 12-month assessments. Generalized estimating equations models were conducted to examine the differential treatment effects of the Breathmobile and FACI compared with standard care.
Results: Children in the combined treatment group (Breathmobile plus FACI) had an increase of 1.7 (6.6%) SFDs that was not maintained at 12 months. In intent-to-treat analyses the FACI-only group had an increase in the number of emergency department visits at 6 months, which was not present at 12 months or in the post hoc as-treated analyses. No significant differences were found between the intervention groups compared with those receiving standard care on all other outcome measures.
Conclusions: Other than a slight improvement in SFDs at 6 months in the Breathmobile plus FACI group, the intervention components did not result in any significant improvements in asthma management or asthma morbidity.
Copyright © 2011 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures

References
-
- McDaniel M, Paxson C, Waldfogel J. Racial disparities in childhood asthma in the United States: evidence from the National Health Interview Survey, 1997 to 2003. Pediatrics. 2006;117(5):e868–e877. - PubMed
-
- Akinbami L. The state of childhood asthma, United States, 1980–2005. Adv Data. 2006;381:1–24. - PubMed
-
- Bravata DM, Sundaram V, Lewis R, Gienger A, Gould MK, McDonald KM, et al. Rockville, MD: Agency for Healthcare Research and Quality; 2007. Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies. Report No.: 04(07)-005 1–5 ed. - PubMed
-
- Rand CS, Butz AM, Kolodner K, Huss K, Eggleston P, Malveaux F. Emergency department visits by urban African American children with asthma. J Allergy Clin Immunol. 2000;105(1 Pt 1):83–90. - PubMed
-
- Sarver N, Murphy K. Management of asthma: new approaches to establishing control. J Am Acad Nurse Pract. 2009;21(1):54–65. - PubMed
