

Adherence to inhaled corticosteroids: an ancillary study of the Childhood Asthma Management Program clinical trial
- PMID: 22104610
- PMCID: PMC3350797
- DOI: 10.1016/j.jaci.2011.10.030
Adherence to inhaled corticosteroids: an ancillary study of the Childhood Asthma Management Program clinical trial
Abstract
Background: Information comparing subjective and objective measurements of adherence to study medications and the effects of adherence on treatment-related differences in asthma clinical trials are limited.
Objective: We sought to compare subjective and objective measurements of children's adherence to inhaled corticosteroids or placebo and to determine whether adherence to study medications modified treatment-related differences in outcomes.
Methods: In an ancillary study conducted in 3 of 8 Childhood Asthma Management Program Clinical Centers, adherence was assessed by using self-reported and objective data in 5- to 12-year-old children with mild or moderate asthma who were randomly assigned to 200 μg of inhaled budesonide twice per day (n = 84) or placebo (n = 56) for 4 years. The κ statistic was used to evaluate agreement between self-reported adherence (daily diary cards) and objectively measured adherence (number of doses left in study inhalers). Multivariable analyses were used to determine whether adherence to study treatment modified treatment-related differences in outcomes.
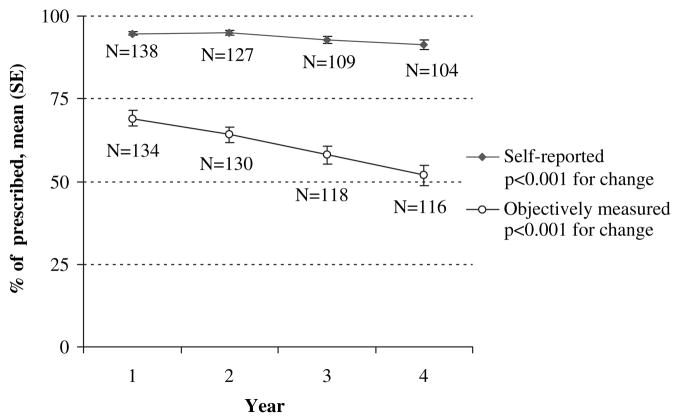
Results: Adherence of less than 80% was seen in 75% of 140 children when adherence was measured objectively but only in 6% of children when measured by means of self-report. There was poor agreement between objective and subjective measurements of adherence of at least 80% (κ = 0.00; 95% CI, -0.05 to 0.04); self-reported adherence over the 4-year period generally overestimated objectively measured adherence (93.6% vs 60.8%, P < .0001). There was little evidence to indicate that adherence modified treatment-related differences in outcomes.
Conclusion: Researchers should use objective rather than self-reported adherence data to identify clinical trial participants with low levels of adherence to study treatment.
Copyright © 2011 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Disclosure of potential conflict of interest: J. A. Krishnan receives research support from the National Institutes of Health (NIH)/National Heart, Lung, and Blood Institute (NHLBI). S. J. Szefler has consultant arrangements with GlaxoSmithKline, Genentech, Merck, Boehringer-Ingelheim, Novartis, and Schering-Plough and receives research support from the NIH/NHLBI’s Childhood Asthma Management Program, the NHLBI’s Childhood Asthma Research and Education, the NIH/NHLBI’s Asthma Clinical Research Network, the NIH/National Institute of Allergy and Infectious Diseases’s Inner City Asthma Consortium, GlaxoSmithKline, National Jewish Health/NHLBI Asthma Net, and the National Institute of Environmental Health Sciences/US Environmental Protection Agency’s Children’s Environmental Health Center grant. R. S. Zeiger has consultant arrangements with AstraZeneca, Aerocrine, Genentech, Merck and Co, Schering-Plough, MedImmune, Sunovion, and Centocor and receives research support from Aerocrine, Genentech, Merck and Co, and GlaxoSmithKline. R. A. Wise has consultant arrangements with AstraZeneca. C. S. Rand is an advisor for the Merck Foundation/MCAN and has consultant arrangements with TEVA. The rest of the authors declare that they have no relevant conflicts of interest.
Figures
References
-
- Martinez FD. Present and future treatment of asthma in infants and young children. J Allergy Clin Immunol. 1999;104:169–74. - PubMed
-
- Dixon AE, Irvin CG. Early intervention of therapy in asthma. Curr Opin Pulm Med. 2005;11:51–5. - PubMed
-
- Verberne AA, Frost C, Roorda RJ, van der Laag H, Kerrebijn KF. One year treatment with salmeterol compared with beclomethasone in children with asthma. The Dutch Pediatric Asthma Study Group. Am J Respir Crit Care Med. 1997;156:685–7. - PubMed
-
- Simons FE. A comparison of beclomethasone, salmeterol, and placebo in children with asthma. Canadian Beclomethasone Diproprionate-Salmeterol Xinafoate Study Group. N Engl J Med. 1997;337:1659–65. - PubMed
-
- The Childhood Asthma Management Program Research Group. Long-term effects of budesonide or nedocromil in children with asthma. N Engl J Med. 2000;343:1054–63. - PubMed
