

Mode of delivery in nulliparous women and neonatal intracranial injury
- PMID: 22105252
- PMCID: PMC3725462
- DOI: 10.1097/AOG.0b013e31823835d3
Mode of delivery in nulliparous women and neonatal intracranial injury
Abstract
Objective: To compare neonatal neurologic complication rates of cesarean deliveries, forceps-assisted vaginal deliveries, and vacuum-assisted vaginal deliveries.
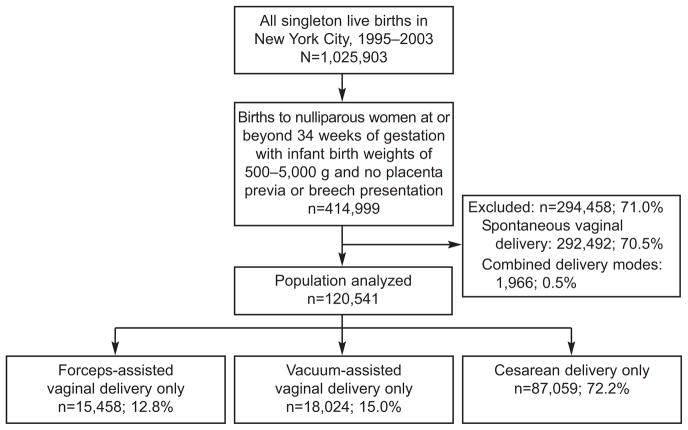
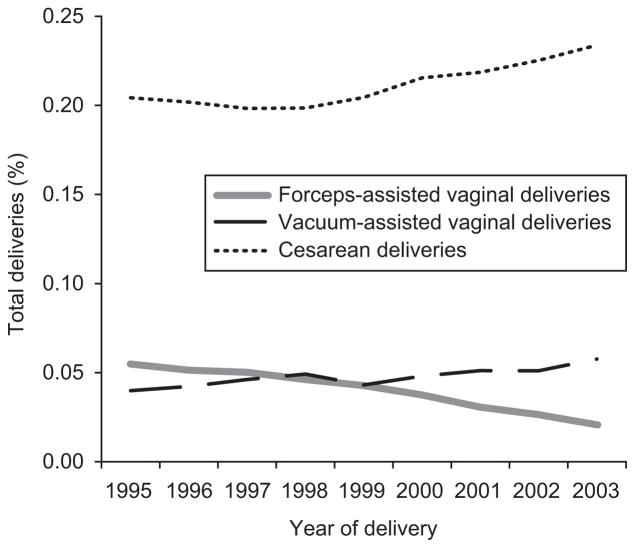
Methods: Data on singleton live births at 34 weeks or greater gestation born to nulliparous women from 1995 to 2003 in New York City were linked to hospital discharge data. Any diagnosis of neonatal subdural hemorrhage, intraventricular hemorrhage, seizures, scalp laceration or cephalohematoma, fracture, facial nerve palsy, brachial plexus injury, or 5-minute Apgar score of less than 7 was considered significant. Multivariable logistic regression was used to estimate associations between delivery mode and these neonatal morbidities.
Results: Forceps-assisted vaginal deliveries were associated with significantly fewer seizures and 5-minute Apgar scores less than 7 compared with vacuum-assisted vaginal deliveries and cesarean deliveries. Cesarean deliveries were linked to less subdural hemorrhages compared with forceps-assisted vaginal deliveries or vacuum-assisted vaginal deliveries. When seizure, intraventricular hemorrhage, and subdural hemorrhage were examined collectively to best predict neurologic outcome, forceps-assisted vaginal deliveries had an overall reduced risk compared with both vacuum-assisted vaginal deliveries (odds ratio [OR] 0.60, 95% confidence interval [CI] 0.40-0.90) and cesarean deliveries (OR 0.68, 95% CI 0.48-0.97). The number needed to treat to prevent one case of severe neurologic morbidity is 509 for forceps-assisted vaginal deliveries compared with vacuum-assisted vaginal deliveries and 559 for forceps-assisted vaginal deliveries compared with cesarean deliveries.
Conclusion: Compared with vacuum-assisted vaginal delivery or cesarean delivery, a forceps-assisted vaginal delivery is associated with a reduced risk of adverse neonatal neurologic outcomes.
Level of evidence: II.
Figures
References
-
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Mathews TJ, Kirmeyer S, et al. Births: final data for 2007. Natl Vital Stat Rep. 2010;58:1–85. - PubMed
-
- Menacker F, Martin JA. Expanded health data from the new birth certificate, 2005. Natl Vital Stat Rep. 2008;58:1–24. - PubMed
-
- Yeomans ER. Operative vaginal delivery. Obstet Gynecol. 2010;115:645–53. - PubMed
-
- Localio AR, Lawthers AG, Bengtson JM, Hebert LE, Weaver SL, Brennan TA, et al. Relationship between malpractice claims and cesarean delivery. JAMA. 1993;269:366–73. - PubMed
-
- Towner D, Castro MA, Eby-Wilkens E, Gilbert WM. Effect of mode of delivery in nulliparous women on neonatal intracranial injury. N Engl J Med. 1999;341:1709–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
