

Clinical subtypes of premenstrual syndrome and responses to sertraline treatment
- PMID: 22105258
- PMCID: PMC3222869
- DOI: 10.1097/AOG.0b013e318236edf2
Clinical subtypes of premenstrual syndrome and responses to sertraline treatment
Abstract
Objective: To estimate response of diagnosis and symptom-based subtypes to sertraline treatment.
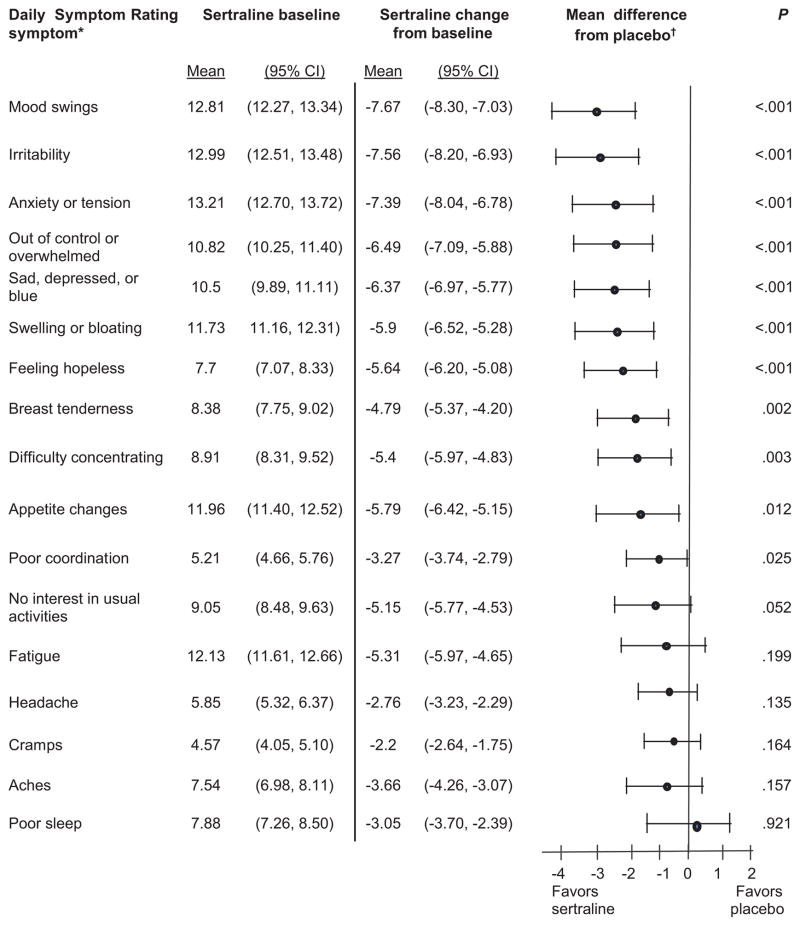
Methods: This was a secondary data analysis for women who were diagnosed with premenstrual syndrome (PMS) or premenstrual dysphoric disorder and treated in three National Institutes of Health-supported clinical trials (N=447). Three PMS subtypes were identified based on predominance of psychological, physical, or both symptom types. Scores for each symptom and a total premenstrual score at baseline and endpoint were calculated from daily symptom diaries. Change from baseline after three treated menstrual cycles (or endpoint if sooner) was estimated using linear regression models adjusted for baseline severity.
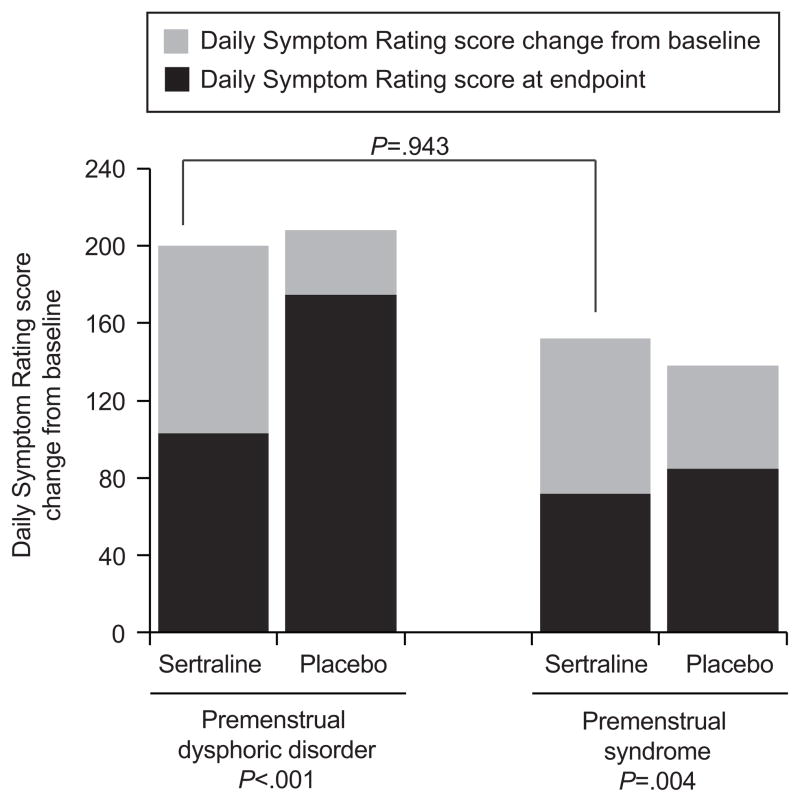
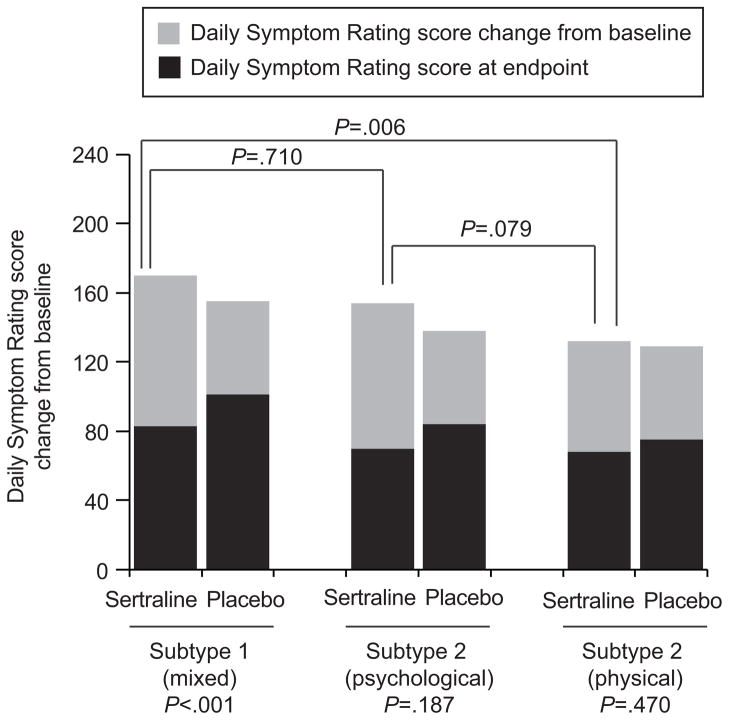
Results: The PMS and premenstrual dysphoric disorder diagnoses improved similarly with sertraline relative to placebo, whereas symptom-based subtypes had differential responses to treatment. The mixed symptom subtype had the strongest response to sertraline relative to placebo (Daily Symptom Rating difference 33.80; 95% confidence interval [CI] 17.16-50.44; P<.001), and the physical symptom subtype had the poorest response to sertraline (Daily Symptom Rating difference 9.50; 95% CI -16.29 to 35.28; P=.470). Results based on clinical improvement (50% decrease from baseline) indicated that 8.3 participants in the mixed symptom subtype, 3.9 in the psychological subtype, and 7.1 in the physical subtype are needed to observe one woman in the subtype who would achieve clinical improvement.
Conclusion: The PMS and premenstrual dysphoric disorder diagnoses have similar response to sertraline treatment, but symptom-based subtypes have significantly different responses to this treatment. Mixed and psychological symptom subtypes improved whereas the physical symptom subtype did not improve significantly. Identifying the patient's predominant symptoms and their severity is important for individualized treatment and a possible response to a selective serotonin reuptake inhibitor.
Level of evidence: II.
Figures
References
-
- Halbreich U, Borenstein J, Pearlstein T, Kahn LS. The prevalence, impairment, impact, and burden of premenstrual dysphoric disorder (PMS/PMDD) Psychoneuroendocrinology. 2003;28:1–23. - PubMed
-
- Dimmock PW, Wyatt KM, Jones PW, O’Brien PM. Efficacy of selective serotonin reuptake inhibitors in premenstrual syndrome: a systematic review. Lancet. 2000;30(356):1131–6. - PubMed
-
- Brown J, O’Brien PM, Marjoribanks J, Wyatt K. Selective serotonin reuptake inhibitors for premenstrual syndrome. Cochrane Database Syst Rev. 2009;2:CD001396. - PubMed
-
- Mitwally MF, Kahn LS, Halbreich U. Pharmacotherapy of premenstrual syndromes and premenstrual dysphoric disorder: current practices. Expert Opin Pharmacother. 2002;3:1577–90. - PubMed
-
- Halbreich U, O’Brien PM, Eriksson E, Bäckström T, Yonkers KA, Freeman EW. Are there differential symptom profiles that improve in response to different pharmacological treatments of premenstrual syndrome/premenstrual dysphoric disorder? CNS Drugs. 2006;20:523–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
