

Continuation rates and complications of intrauterine contraception in women diagnosed with bipolar disorder
- PMID: 22105263
- PMCID: PMC3228274
- DOI: 10.1097/AOG.0b013e318233beae
Continuation rates and complications of intrauterine contraception in women diagnosed with bipolar disorder
Abstract
Objective: To estimate continuation rates, complications, and psychiatric hospitalizations among women with bipolar disorder using levonorgestrel-releasing or copper-containing intrauterine devices (IUDs) as compared with those using depot medroxyprogesterone acetate or sterilization for birth control.
Methods: Data for this cohort study were obtained from a nationwide health insurance claims database on an employed, commercially insured population. Women aged 18-44 years with a prior diagnosis of bipolar disorder (n=849) who were using the levonorgestrel intrauterine system, a copper-containing IUD, depot medroxyprogesterone acetate, or sterilization were evaluated. Outcomes included continuation rates over a 12-month interval, infectious and noninfectious complications, and hospitalizations for bipolar disorder or depression.
Results: Women using an IUD were more likely than those using depot medroxyprogesterone acetate to continue the method for at least 12 months (copper-containing IUD, 86%; levonorgestrel intrauterine system, 87%). In comparison, only 31% of those who initiated depot medroxyprogesterone acetate received three more injections during the next year (P<.001). No significant differences were noted in infectious or noninfectious complications by contraceptive type. Finally, no differences were observed in the number of hospitalizations for bipolar disorder or depression among the four contraceptive groups.
Conclusion: More women with bipolar disorder continued using IUDs at one year than women using depot medroxyprogesterone acetate. The rates of complications and psychiatric hospitalizations were not different among women using an IUD, depot medroxyprogesterone acetate, or sterilization.
Level of evidence: II.
Conflict of interest statement
Figures
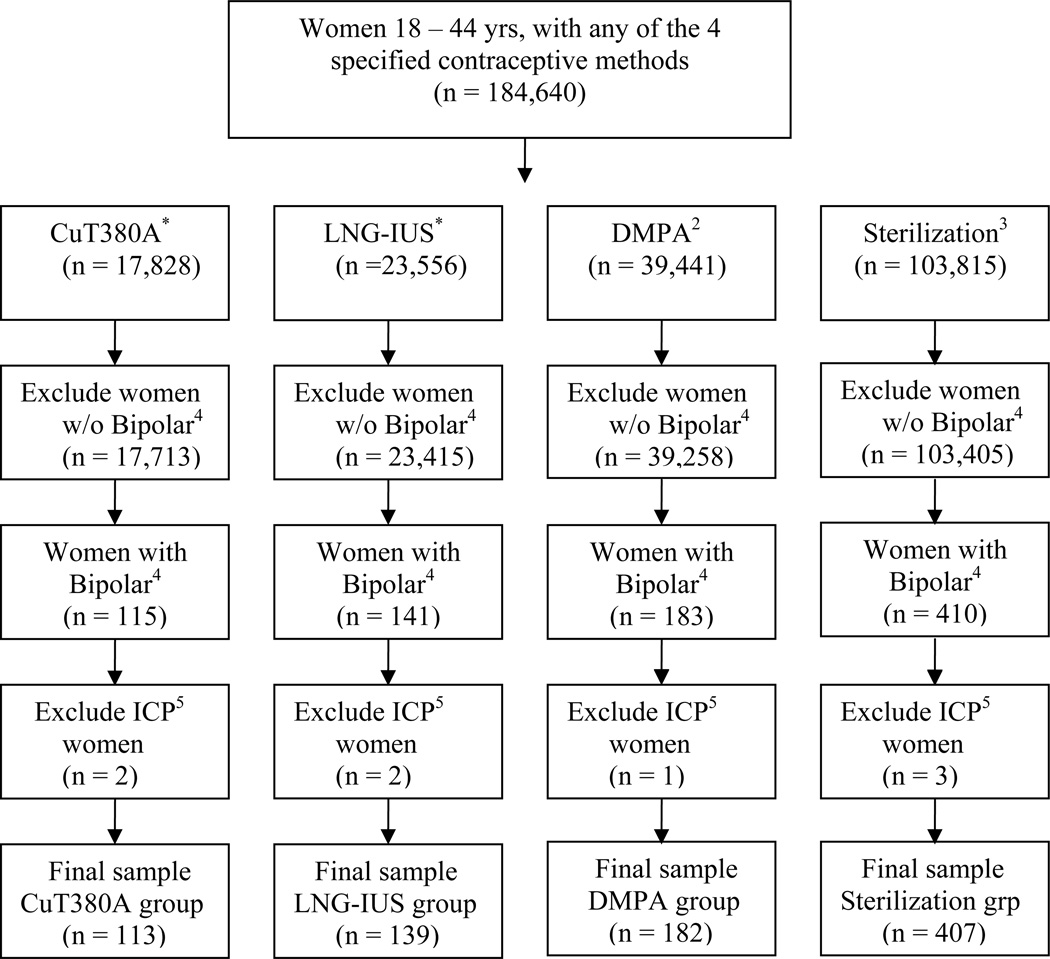
Women with a LNG-IUS insertion were identified as those who had (a) HCPCS codes of S4981 or J7302, and any of the following CPT or ICD-9 codes: 58300, 69.7, V25.1 and V25.42. Women with a CuT380A insertion were identified as those who had HCPCS code of J7300, and any of the following: CPT code of 88300 or ICD-9-CM codes of 69.7, V25.1 and V25.42.
A woman was classified in the DMPA group if she received 4 injections in a 12-month period. The HCPCS code of J1055 was used to identify DMPA injection.
The codes for sterilization included: CPT codes of 58565, 58600, 58605, 58611, 58615, 58670, 58671, and ICD-9-CM codes of 66.2, 66.3, V25.2.
The diagnosis codes for bipolar disorder (BPD-I, BPD-II, BPD-Not Otherwise Specified (NOS)/subthreshold) include 296.0-296.8 except for codes 296.2 and 296.3. We included only those diagnoses by a mental health professional.
The diagnosis codes for women who were immunocompromised (ICP) include: 042, 043, 044, 279.0-279.3.
Similar articles
-
HIV incidence among women using intramuscular depot medroxyprogesterone acetate, a copper intrauterine device, or a levonorgestrel implant for contraception: a randomised, multicentre, open-label trial.Lancet. 2019 Jul 27;394(10195):303-313. doi: 10.1016/S0140-6736(19)31288-7. Epub 2019 Jun 13. Lancet. 2019. PMID: 31204114 Free PMC article. Clinical Trial.
-
Effects of depot medroxyprogesterone acetate, the copper IUD and the levonorgestrel implant on testosterone, sex hormone binding globulin and free testosterone levels: ancillary study of the ECHO randomized clinical trial.BMC Womens Health. 2024 Mar 8;24(1):167. doi: 10.1186/s12905-024-02990-8. BMC Womens Health. 2024. PMID: 38459552 Free PMC article. Clinical Trial.
-
Contraceptive method preference and reasons for contraceptive discontinuation among women randomized to intramuscular depot medroxyprogesterone acetate, a copper intrauterine device or a levonorgestrel implant: Findings from Durban, South Africa.Contraception. 2022 Apr;108:37-43. doi: 10.1016/j.contraception.2021.11.002. Epub 2021 Nov 27. Contraception. 2022. PMID: 34848180 Clinical Trial.
-
Intrauterine devices. The optimal long-term contraceptive method?J Reprod Med. 1999 Mar;44(3):269-74. J Reprod Med. 1999. PMID: 10202746 Review.
-
Long-acting contraceptive options.Int J Fertil Menopausal Stud. 1996 Mar-Apr;41(2):69-76. Int J Fertil Menopausal Stud. 1996. PMID: 8829701 Review.
Cited by
-
Contraception counseling for women with premenstrual dysphoric disorder (PMDD): current perspectives.Open Access J Contracept. 2019 Sep 20;10:27-39. doi: 10.2147/OAJC.S183193. eCollection 2019. Open Access J Contracept. 2019. PMID: 31572029 Free PMC article.
-
Pharmacists and Contraception in the Inpatient Setting.Pharmacy (Basel). 2020 May 9;8(2):82. doi: 10.3390/pharmacy8020082. Pharmacy (Basel). 2020. PMID: 32397460 Free PMC article.
-
Women with Schizophrenia over the Life Span: Health Promotion, Treatment and Outcomes.Int J Environ Res Public Health. 2020 Aug 3;17(15):5594. doi: 10.3390/ijerph17155594. Int J Environ Res Public Health. 2020. PMID: 32756418 Free PMC article. Review.
-
Safety of hormonal contraception and intrauterine devices among women with depressive and bipolar disorders: a systematic review.Contraception. 2016 Dec;94(6):641-649. doi: 10.1016/j.contraception.2016.06.012. Epub 2016 Jun 27. Contraception. 2016. PMID: 27364100 Free PMC article.
-
Impulsivity, Unplanned Pregnancies, and Contraception Among Women with Bipolar Disorder.Neuropsychiatr Dis Treat. 2020 Feb 7;16:407-414. doi: 10.2147/NDT.S238887. eCollection 2020. Neuropsychiatr Dis Treat. 2020. PMID: 32103960 Free PMC article.
References
-
- Kessler RC, Merikangas KR, Wang PS. Prevalence, comorbidity, and service utilization for mood disorders in the United States at the beginning of the twenty-first century. Annu Rev Clin Psychol. 2007;3:137–158. - PubMed
-
- National Comorbidity Survey Replication (NCS-R) [Accessed 05/24/2011];12-month prevalence estimates. 2007 Table 2. Available at http://www.hcp.med.harvard.edu/ncs/
-
- Magalhães PV, Kapczinski F, Kauer-Sant'Anna M. Use of contraceptive methods among women treated for bipolar disorder. Arch Womens Ment Health. 2009;12:183–185. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
