

Thymic malignancies: from clinical management to targeted therapies
- PMID: 22105817
- PMCID: PMC3675690
- DOI: 10.1200/JCO.2011.36.0487
Thymic malignancies: from clinical management to targeted therapies
Abstract
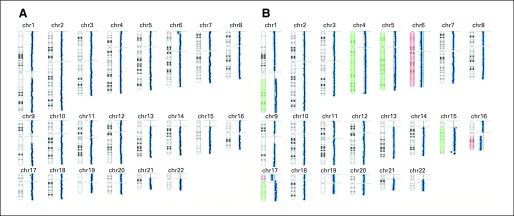
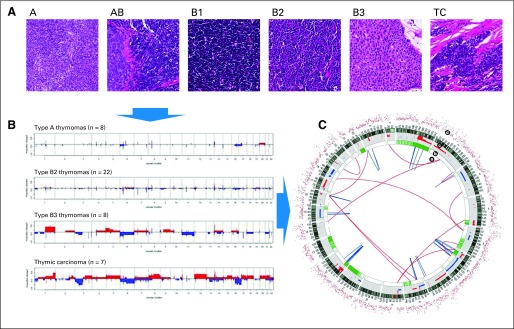
Purpose: A key challenge in the treatment of thymoma and thymic carcinoma (TC) is in improving our understanding of the molecular biology of these relatively rare tumors. In recent years, significant efforts have been made to dissect the molecular pathways involved in their carcinogenesis. Here we discuss the results of large-scale genomic analyses conducted to date and review the most active chemotherapies and targeted treatments.
Methods: We reviewed the literature for chemotherapeutic trials in the last 20 years and trials involving targeted therapies between 1999 and 2010. The search was supplemented by a review of abstracts presented at the annual meetings of the American Society of Clinical Oncology (from 1999 to 2010), at the first International Conference on Thymic Malignancies in 2009, and at a follow-up meeting of the newly formed International Thymic Malignancies Interest Group in 2010.
Results: Surgery remains the treatment of choice for operable tumors, whereas chemotherapy is standard in locally advanced and metastatic disease. Thus far, targeted therapies have been developed empirically. Histone deacetylase inhibitors have shown some activity in thymoma whereas sunitinib may be active in TC. There are no data to support the use of HER2- or EGFR-targeted therapies in thymic malignancies.
Conclusion: Drug development for the treatment of thymic malignancies is difficult because of the rarity of these tumors. Ethnic differences are becoming apparent, with aggressive subtypes being observed in Asians and African Americans. Incremental improvements in our understanding of tumor biology suggest that molecular profiling-directed therapies may be the preferred route of investigation in the future.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Margaritora S, Cesario A, Cusumano G, et al. Thirty-five-year follow-up analysis of clinical and pathologic outcomes of thymoma surgery. Ann Thorac Surg. 2010;89:245–252. discussion 252. - PubMed
-
- Engels EA, Pfeiffer RM. Malignant thymoma in the United States: Demographic patterns in incidence and associations with subsequent malignancies. Int J Cancer. 2003;105:546–551. - PubMed
-
- Evoli A, Punzi C, Marsili F, et al. Extrathymic malignancies in patients with thymoma. Ann Oncol. 2004;15:692–693. - PubMed
-
- Pan CC, Chen PC, Wang LS, et al. Thymoma is associated with an increased risk of second malignancy. Cancer. 2001;92:2406–2411. - PubMed
-
- Loehrer PJ, Sr, Wang W, Johnson DH, et al. Octreotide alone or with prednisone in patients with advanced thymoma and thymic carcinoma: An Eastern Cooperative Oncology Group Phase II Trial. J Clin Oncol. 2004;22:293–299. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
