

Anatomical distribution of vertebral fractures: comparison of pediatric and adult spines
- PMID: 22109742
- PMCID: PMC4067402
- DOI: 10.1007/s00198-011-1837-1
Anatomical distribution of vertebral fractures: comparison of pediatric and adult spines
Abstract
Summary: We compared the distribution of vertebral fractures in adults and children and found that fractures occurred in different locations in the two age groups. This likely relates to the different shape of the immature spine.
Introduction: We hypothesized that the anatomical distribution of vertebral fractures (VF) would be different in children compared to adults.
Methods: We compared the distribution of VF defined using the Genant semi-quantitative method (GSQ method) in adults (N = 221; 545 fractures) and in children early in the course of glucocorticoid therapy (N = 44; 94 fractures).
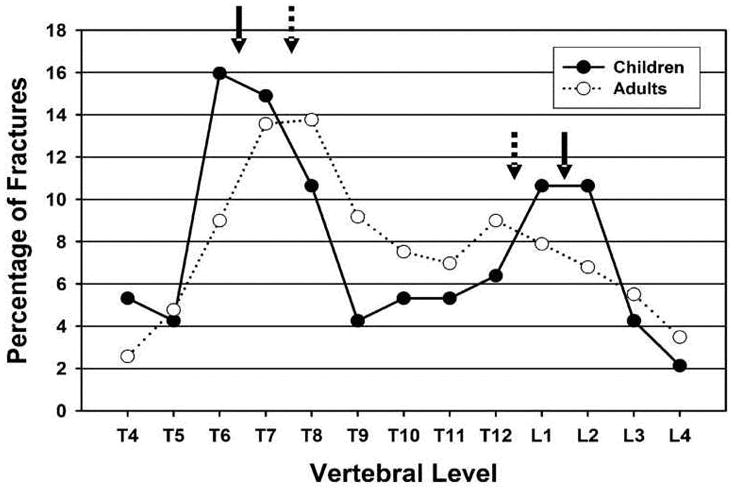
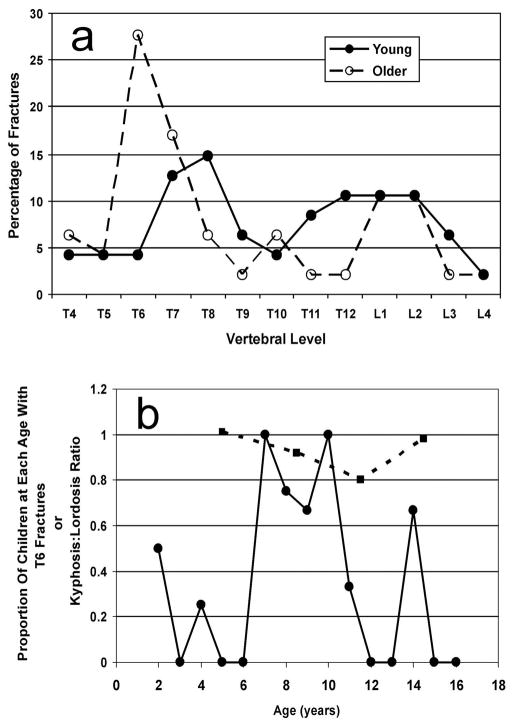
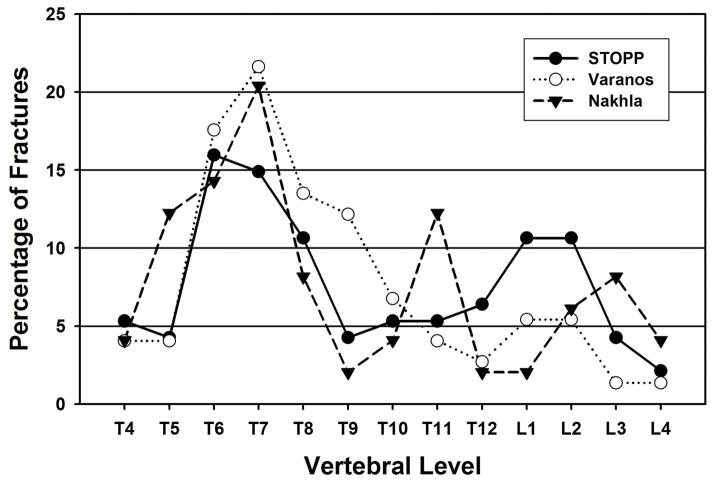
Results: The average age in the adult cohort was 62.9 years (standard deviation (SD), 13.4 years), 26% was male, the mean lumbar spine Z-score was -1.0 (SD, 1.5), and the corresponding T-score was -2.4 (SD, 1.4). The pediatric cohort median age was 7.7 years (range, 2.1-16.6 years), the mean lumbar spine Z-score was -1.7 (SD, 1.5), 52% was male, and disease categories were acute lymphoblastic leukemia (66%), rheumatological conditions (21%), and nephrotic syndrome (14%). The VF distribution was biphasic in both populations, but the peaks differed in location. In adults, the peaks were at T7/T8 and at T12/L1. In children, the focus was higher in the thoracic spine, at T6/T7, and lower in the lumbar spine, at L1/L2. When children were assessed in two age-defined sub-groups, a biphasic VF distribution was seen in both, but the upward shift of the thoracic focus to T6 was observed only in the older group, with the highest rates of fracture present between ages 7 and 10 years.
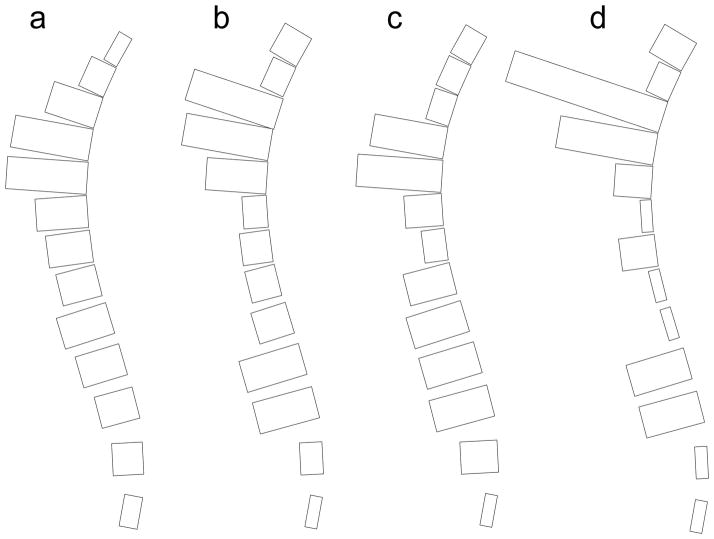
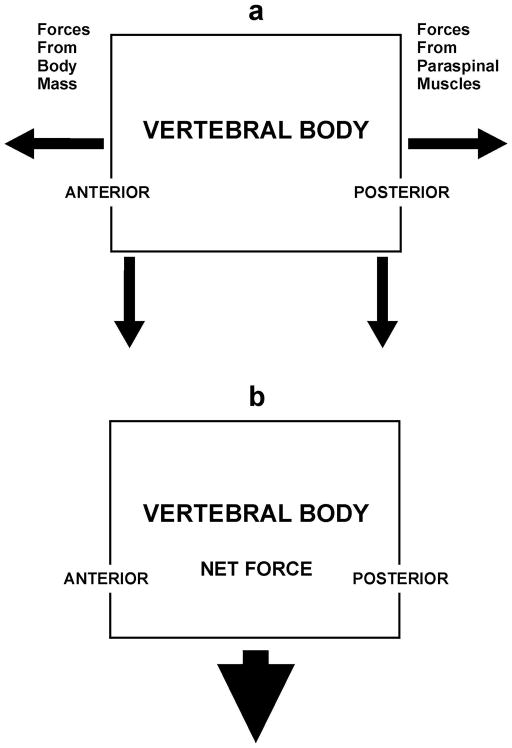
Conclusions: These results suggest that the anatomical distribution of VF differs between children and adults, perhaps relating to the different shape of the immature spine, notably the changing ratio of kyphosis to lordosis.
Conflict of interest statement
Figures
References
-
- Silva MJ. Biomechanics of osteoporotic fractures. Injury. 2007;38S3:S69–S76. - PubMed
-
- Zebaze R, Maalouf G, Maalouf N, Seeman E. Loss of regularity in the curvature of the thoracolumbar spine: a measure of structural failure. J Bone Miner Res. 2004;19:1099–1104. - PubMed
-
- Legaye J, Duval-Beaupere G. Sagittal plane alignment of the spine and gravity. A radiological and clinical evaluation. Acta Orthop Belg. 2005;71:213–220. - PubMed
-
- Cil A, Yazici M, Uzumcugil A, et al. The evolution of sagittal segmental alignment of the spine during childhood. Spine. 2004;30:93–100. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
