

Quantitative histological-hemodynamic correlations in cirrhosis
- PMID: 22109744
- PMCID: PMC3721182
- DOI: 10.1002/hep.24805
Quantitative histological-hemodynamic correlations in cirrhosis
Abstract
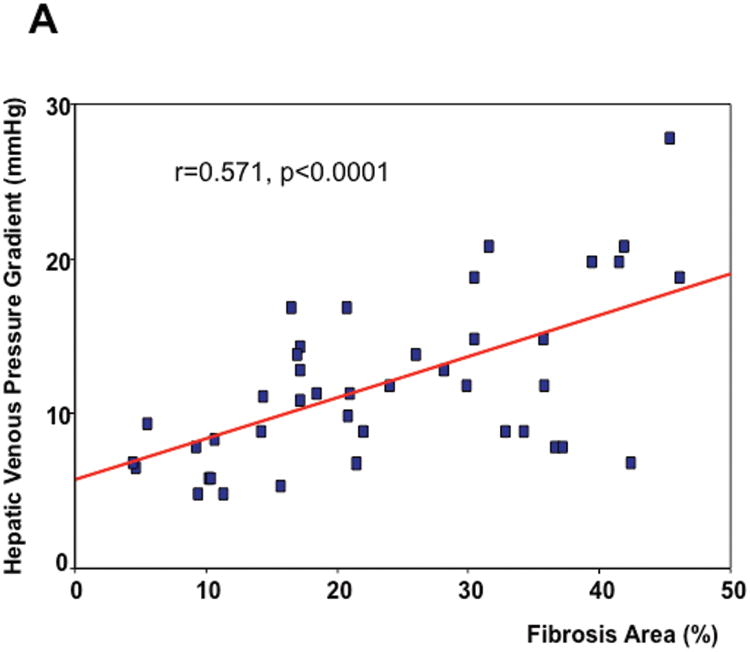
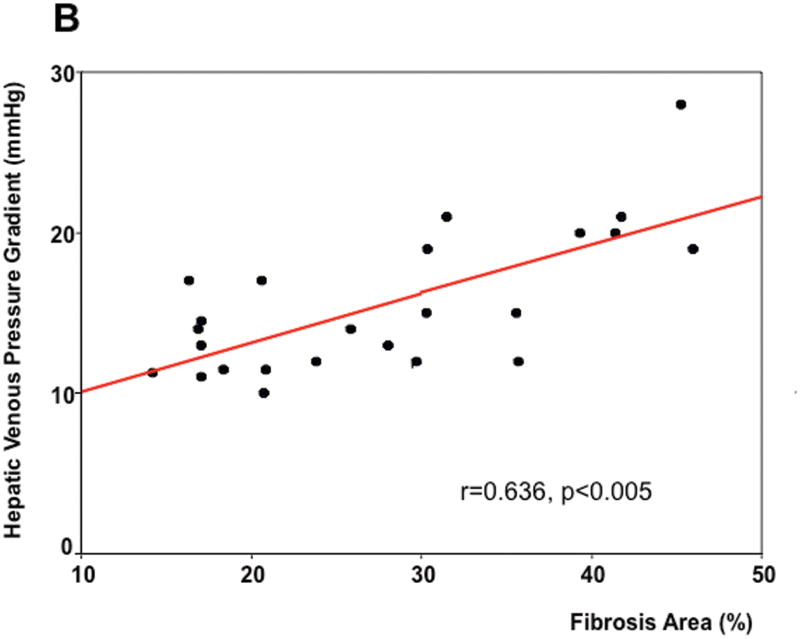
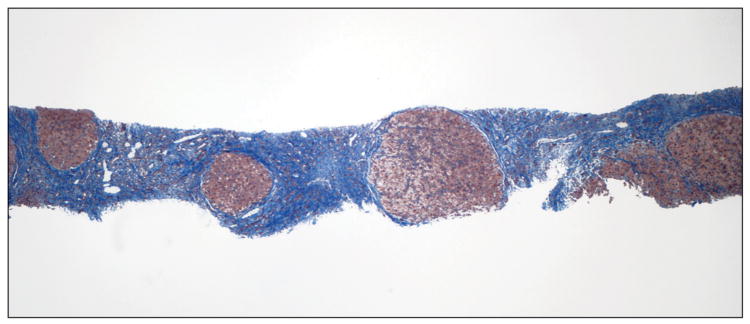
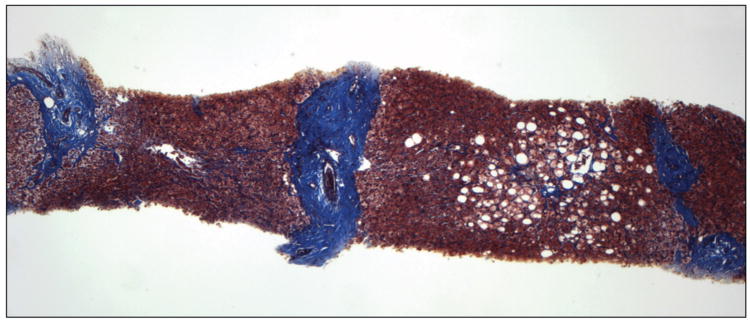
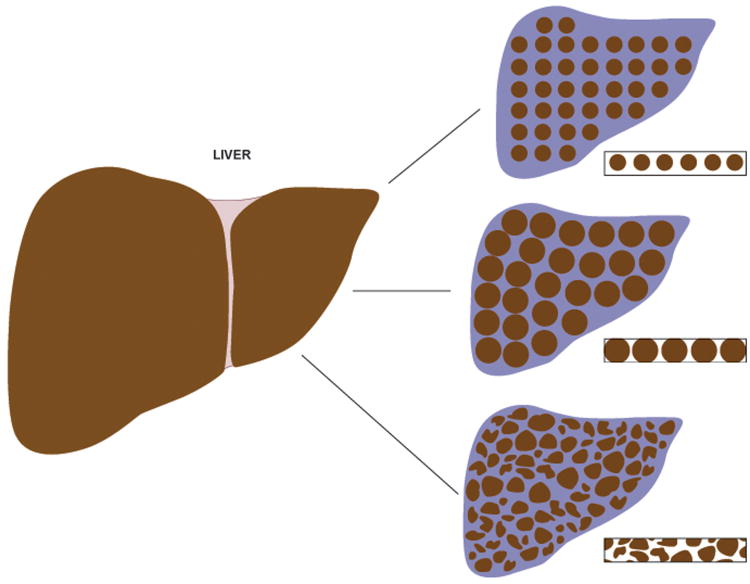
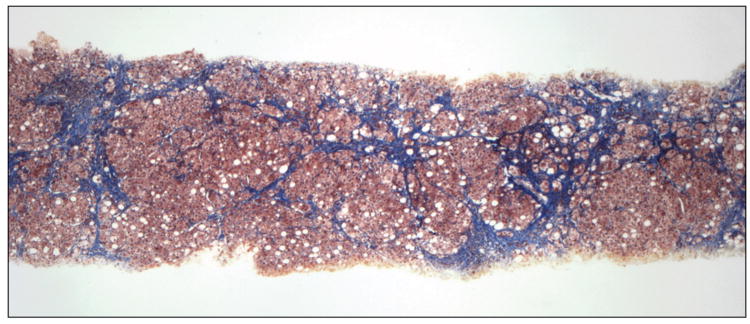
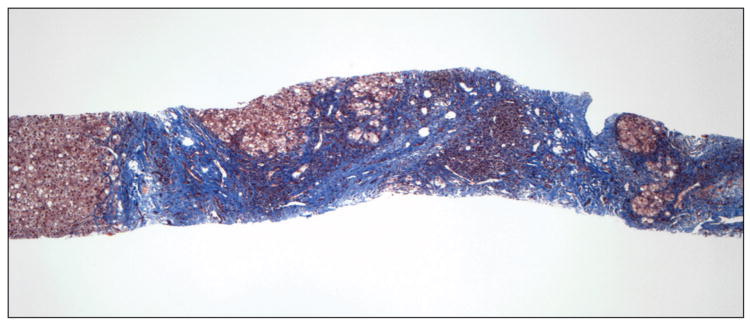
We have previously shown, in a semiquantitative analysis of liver biopsies showing cirrhosis, that thickness of fibrous septa separating cirrhotic nodules and small size of cirrhotic nodules correlated independently with portal pressure (as determined by the hepatic venous pressure gradient; HVPG) and were independent predictors of the presence of clinically significant portal hypertension (PH). This study aimed to confirm these results using quantitative analysis of these biopsies using digital image analysis. Biopsies of 42 patients with cirrhosis and HVPG measurements within 6 months of the biopsy were included in the study. The following parameters were scored quantitatively and without knowledge of HVPG results: total fibrosis area, septal thickness, nodule size, and number of nodules per millimeter of length of liver biopsy. Fibrosis area was the only parameter that independently correlated with HVPG (r = 0.606; P < 0.0001). Correlation was significant, even among patients with clinically significant PH (r = 0.636; P < 0.005). Fibrosis area and nodule size were both independently predictive of the presence of clinically significant PH (r = 0.57; P = 0.003).
Conclusions: On quantitative analysis, fibrosis area was the parameter that correlated best with HVPG and the presence of clinically significant PH. Beyond pathophysiological implications, this also has methodological implications that are discussed in this article.
Copyright © 2011 American Association for the Study of Liver Diseases.
Figures

References
-
- Groszmann RJ, Garcia-Tsao G, Bosch J, et al. Beta-blockers to prevent gastroesophageal varices in patients with cirrhosis. N Engl J Med. 2005;353:2254–2261. - PubMed
-
- Ripoll C, Groszmann R, Garcia-Tsao G, et al. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology. 2007;133:481–488. - PubMed
-
- D'Amico G, Garcia-Tsao G, Cales P, Escorsell A, Nevens F, Cestari R, Caletti G, Zoli M. Diagnosis of portal hypertension: how and when. In: DeFranchis R, editor. Portal Hypertension III; Proceedings of the Third Baveno International Consensus Workshop on Definitions, Methodology and Therapeutic Strategies; Oxford. Blackwell Science; 2001. pp. 36–64.
-
- Nagula S, Jain D, Groszmann R, et al. Histological-hemodynamic correlation in cirrhosis-a histological classification of the severity of cirrhosis. J Hepatol. 2006;44:111–117. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical