

Phenomenological features and clinical impact of affective disorders in OCD: a focus on the bipolar disorder and OCD connection
- PMID: 22109969
- PMCID: PMC3322278
- DOI: 10.1002/da.20908
Phenomenological features and clinical impact of affective disorders in OCD: a focus on the bipolar disorder and OCD connection
Abstract
Background: Given the general population prevalence rates of obsessive compulsive disorder (OCD) and the affective disorders, one would expect the co-occurrence of these syndromes to be rare. Yet findings by our group and others have revealed extremely high rates of comorbidity in OCD with both depressive disorders (DD; 50%) and bipolar disorder (BPD; 10%). The current investigation sought to further clarify the role affective disorder comorbidity-particularly that with BPD-may play in the clinical expression of OCD.
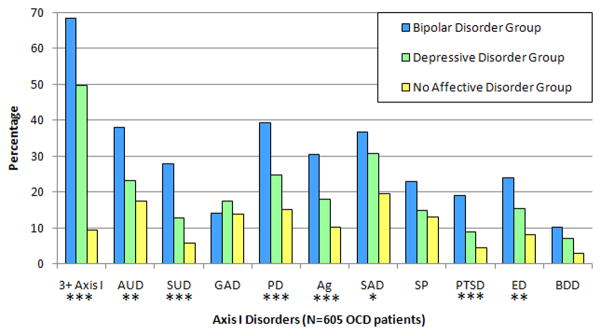
Method: A total of 605 individuals with OCD were evaluated with the Structured Clinical Interview for DSM-IV. The sample included three groups: BPD (bipolar I or II; N = 79, 13.1%), DD (major depression or dysthymia; N = 388, 64.1%), and NAD (no affective disorder comorbidity; N = 138, 22.8%). Group-wise comparisons were conducted on comorbidity patterns, impairment measures, and clinical features of OCD.
Results: Analyses revealed a graded severity pattern, with the BPD group as the most severe, followed by the DD group, and finally the NAD group. Severity was reflected by the total number of Axis I disorders (P<.01), the number of psychiatric hospitalizations (P<.001), impairment measures (Ps<.05), and OCD symptoms (P<.01). It is worth noting that the impairment and OCD symptom severity findings were not attributable to the higher level of nonmood disorder comorbidities in the BPD and DD groups.
Results: Those individuals with comorbid affective disorders, particularly BPD, represent a clinically severe group compared to those without such comorbidity. Clarifying the phenomenological features of OCD-affective disorder comorbidity has important etiological and treatment implications.
© 2011 Wiley Periodicals, Inc.
Figures
References
-
- Olatunji BO, Williams BJ, Haslam N, et al. The latent structure of obsessive-compulsive symptoms: a taxometric study. Depress Anxiety. 2008;25(11):956–68. - PubMed
-
- Angst J, Gamma A, Endrass J, et al. Obsessive-compulsive severity spectrum in the community: prevalence, comorbidity, and course. European Archives of Psychiatry and Clinical Neuroscience. 2004;254(3):156–64. - PubMed
-
- Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey. Replication Archives of General Psychiatry. 2005;62(6):593–602. - PubMed
-
- Lopez AD, Murray CC. The global burden of disease, 1990–2020. Nat Med. 1998;4(11):1241–3. - PubMed
-
- Angst J, Gamma A, Endrass J, et al. Obsessive-compulsive syndromes and disorders: significance of comorbidity with bipolar and anxiety syndromes. Eur Arch Psychiatry Clin Neurosci. 2005;255(1):65–71. - PubMed
