

Effectiveness and limitations of hand hygiene promotion on decreasing healthcare-associated infections
- PMID: 22110610
- PMCID: PMC3217962
- DOI: 10.1371/journal.pone.0027163
Effectiveness and limitations of hand hygiene promotion on decreasing healthcare-associated infections
Abstract
Background: Limited data describe the sustained impact of hand hygiene programs (HHPs) implemented in teaching hospitals, where the burden of healthcare-associated infections (HAIs) is high. We use a quasi-experimental, before and after, study design with prospective hospital-wide surveillance of HAIs to assess the cost effectiveness of HHPs.
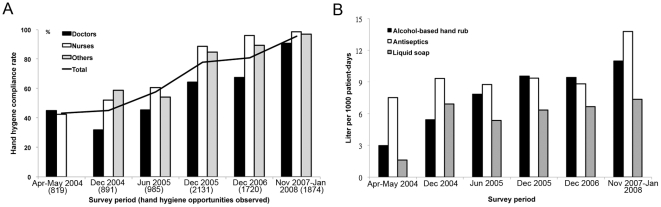
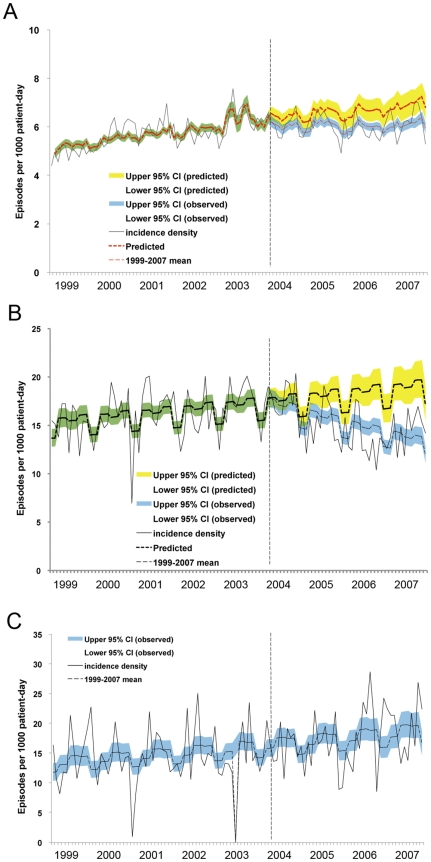
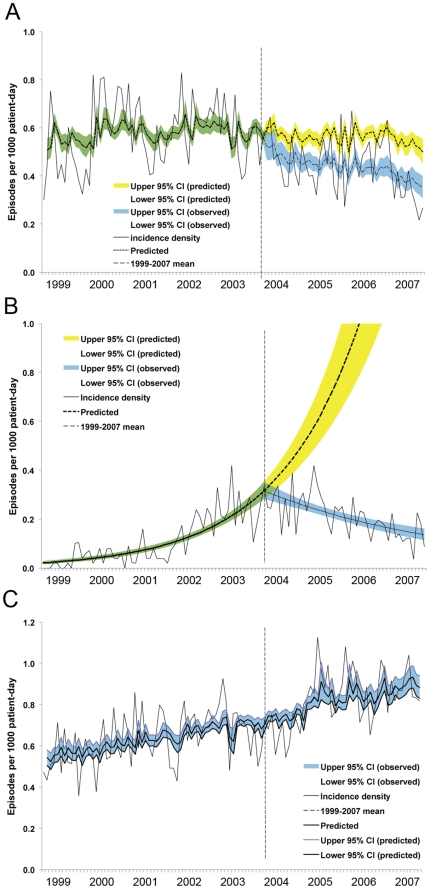
Methods and findings: A 4-year hospital-wide HHP, with particular emphasis on using an alcohol-based hand rub, was implemented in April 2004 at a 2,200-bed teaching hospital in Taiwan. Compliance was measured by direct observation and the use of hand rub products. Poisson regression analyses were employed to evaluate the densities and trends of HAIs during the preintervention (January 1999 to March 2004) and intervention (April 2004 to December 2007) periods. The economic impact was estimated based on a case-control study in Taiwan. We observed 8,420 opportunities for hand hygiene during the study period. Compliance improved from 43.3% in April 2004 to 95.6% in 2007 (p<.001), and was closely correlated with increased consumption of the alcohol-based hand rub (r = 0.9399). The disease severity score (Charlson comorbidity index) increased (p = .002) during the intervention period. Nevertheless, we observed an 8.9% decrease in HAIs and a decline in the occurrence of bloodstream, methicillin-resistant Staphylococcus aureus, extensively drug-resistant Acinetobacter baumannii, and intensive care unit infections. The intervention had no discernable impact on HAI rates in the hematology/oncology wards. The net benefit of the HHP was US$5,289,364, and the benefit-cost ratio was 23.7 with a 3% discount rate.
Conclusions: Implementation of a HHP reduces preventable HAIs and is cost effective.
Conflict of interest statement
Figures
References
-
- Burke JP. Infection Control - A problem for patient safety. N Engl J Med. 2003;348:651–656. - PubMed
-
- World Health Organization. WHO guidelines on hand hygiene in health care. 2009. First global patient safety challenge: clean care is safe care. http://whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf. Accessed May 5, 2010.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
