

Chin ptosis: classification, anatomy, and correction
- PMID: 22110784
- PMCID: PMC3052727
- DOI: 10.1055/s-0028-1098968
Chin ptosis: classification, anatomy, and correction
Abstract
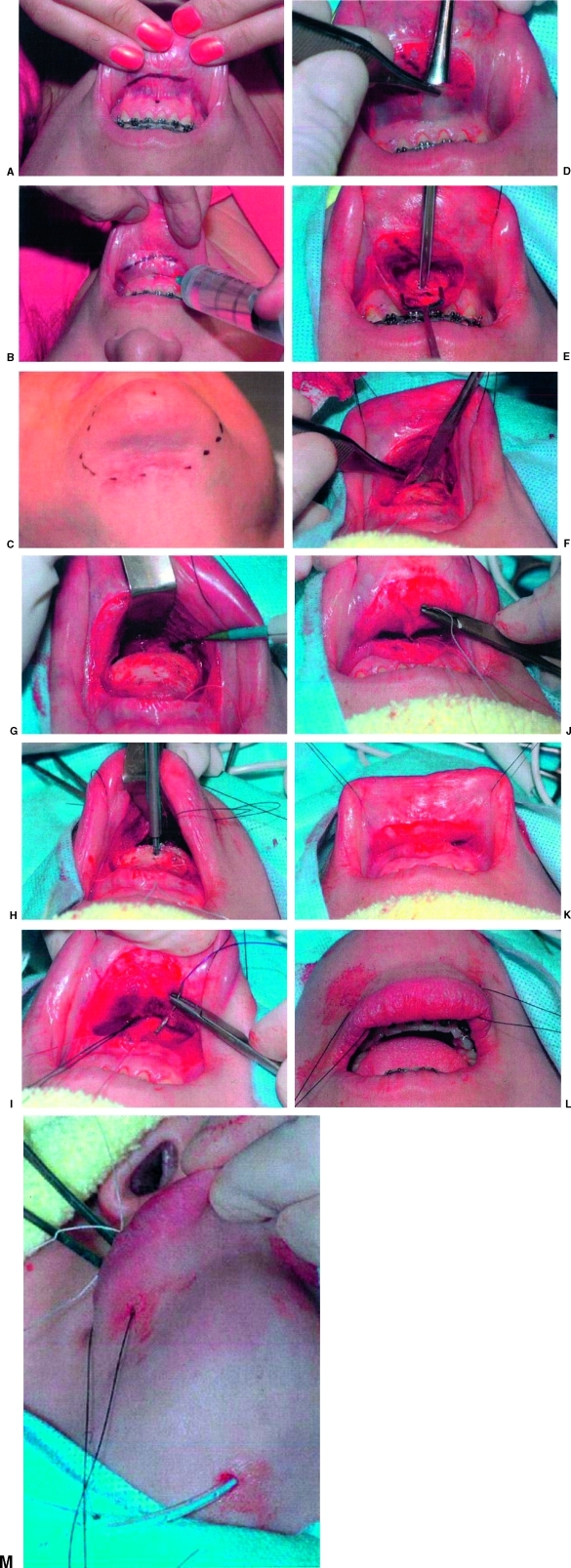
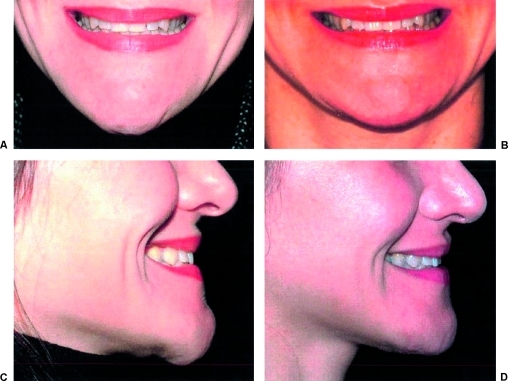
For years, the notion of chin ptosis was somehow integrated with the concept of witch's chin. That was a mistake on many levels because chin droop has four major causes, all different and with some overlap. With this article, the surgeon can quickly diagnose which type and which therapeutic modality would work best. In some cases the problem is a simple fix, in others the droop can only be stabilized, and in the final two, definite corrective procedures are available. Of note, in certain situations two types of chin ptosis may overlap because both the patient and the surgeon may each contribute to the problems. For example, in dynamic ptosis, a droop that occurs with smile in the unoperated patient can be exacerbated and further produced by certain surgical methods also. This paper classifies the variations of the problems and explains the anatomy with the final emphasis on long-term surgical correction, well described herein. This article is the ninth on this subject and a review of them all would be helpful (greatly) for understanding the enigmas of the lower face.
Keywords: Lip incompetence; chin droop; chin ptosis; mentalis muscle; witch's chin.
Figures












References
-
- Zide B M, McCarthy J. The mentalis muscle: an essential component of chin and lower lip position. Plast Reconstr Surg. 1989;83(3):413–420. - PubMed
-
- Zide B M. The mentalis muscle: an essential component of chin and lower lip position. Plast Reconstr Surg. 2000;105(3):1213–1215. - PubMed
-
- González-Ulloa M. Ptosis of the chin: the witches' chin. Plast Reconstr Surg. 1972;50:54–57. - PubMed
-
- Lesavoy M A, Creasman C, Schwartz R I. A technique for correcting witch's chin deformity. Plast Reconstr Surg. 1996;97(4):842–846. - PubMed
-
- Peterson R A. Correction of the senile chin by derma-fat flaps, chin implant, and platysma plication. 1982 Fifteenth Annual Meeting of the American Society for Aesthetic Plastic Surgery. Las Vegas, NV: April 22.
LinkOut - more resources
Full Text Sources
Other Literature Sources