

doi: 10.1055/s-0028-1098963.
Craniofacial Bone Grafting: Wolff's Law Revisited
- PMID: 22110789
- PMCID: PMC3052728
- DOI: 10.1055/s-0028-1098963
Item in Clipboard
Craniofacial Bone Grafting: Wolff's Law Revisited
Craniomaxillofac Trauma Reconstr.
2008 Nov.
Abstract
Bone grafts are used for the reconstruction of congenital and acquired deformities of the facial skeleton and, as such, comprise a vital component of the craniofacial surgeon's armamentarium. A thorough understanding of bone graft physiology and the factors that affect graft behavior is therefore essential in developing a more intelligent use of bone grafts in clinical practice. This article presents a review of the basic physiology of bone grafting along with a survey of pertinent concepts and current research. The factors responsible for bone graft survival are emphasized.
Keywords: Wolff's law; bone graft; mechanotransduction; osteoconduction; osteoinduction.
Figures
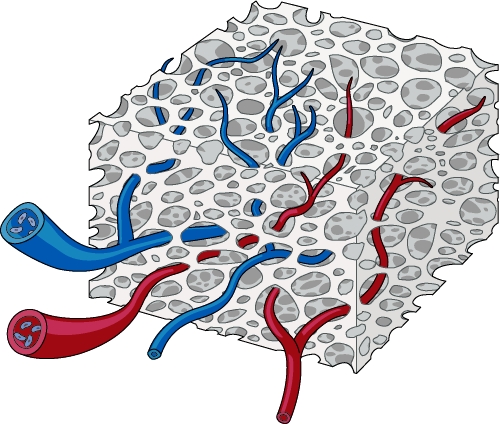
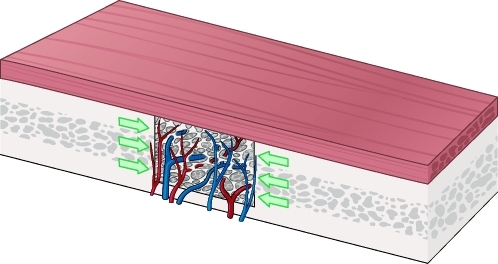
Cancellous bone graft revascularization occurs rapidly and completely, owing to its open architecture.
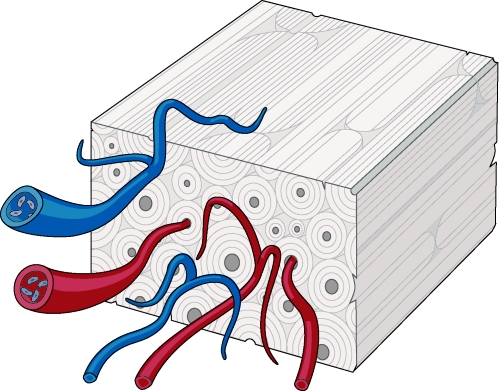
Cortical bone graft revascularization occurs slowly and incompletely, owing to its dense lamellar structure. Vessels must penetrate along haversian and Volkmann's canals.
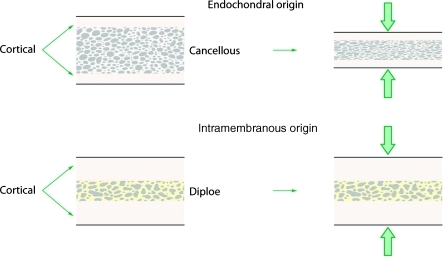
The embryologic origin of a graft is significant only in that it determines the relative proportion of cortical and cancellous bone within the graft. (Adapted from Hardesty RA, Marsh JL. Craniofacial onlay bone grafting: a prospective evaluation of graft morphology, orientation, and embryonic origin. Plast Reconstr Surg 1990;85(1):5–14.)
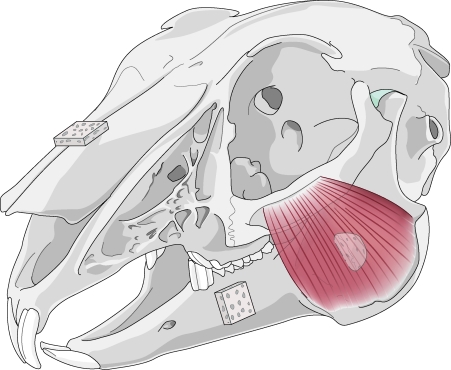
Enlow's theory of resorptive and depository fields asserts that certain areas remodel by bony resorption (mandibular ramus), whereas others remodel by bony deposition (mandibular body and snout), as shown here in the rabbit skull.
Cancellous bone grafts demonstrate favorable remodeling characteristics when placed in the inlay position.
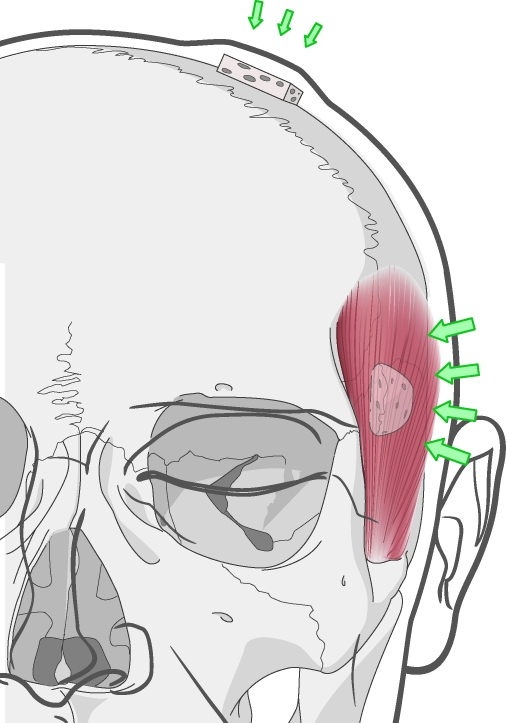
Onlay bone grafting in different regions of the face. Grafts placed under the temporalis muscle experience a greater magnitude of compressive force than those placed under the scalp. Clinically, onlay grafts placed under the temporalis undergo near-complete resorption.
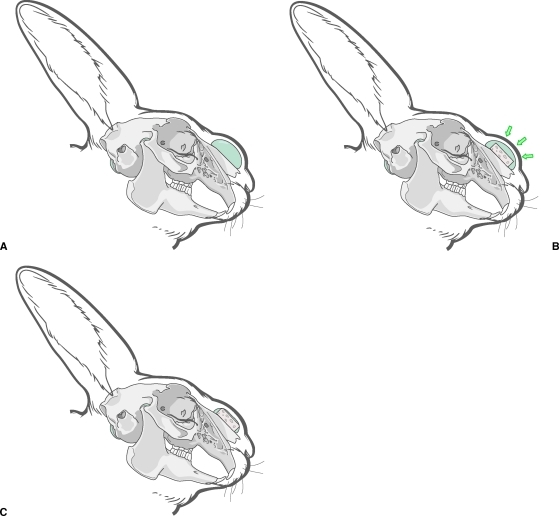
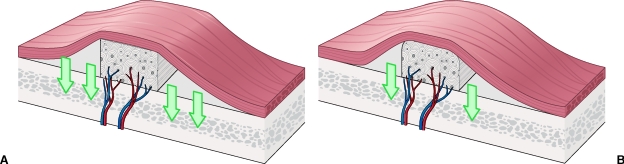
(A–C) A “shielding” effect is demonstrated when tissue expansion proceeds bone grafting. This is hypothesized to reduce the compression forces on the graft, which in turn lead to resorption.
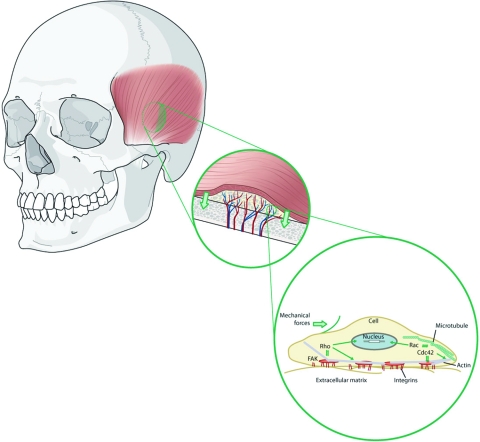
Wolff's law, revisited: mechanotransduction. Mechanical forces induce intracellular signals, which dictate bone graft behavior.
(A,B) Cortical bone grafts are preferred in the onlay position. Their dense structure resists compressive forces and revascularization, both of which would otherwise resorb the graft.
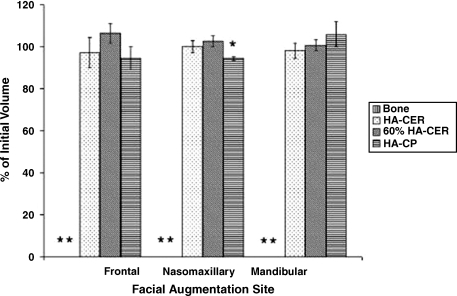
Comparison of autologous bone grafts to hydroxyapatite composite grafts in various regions of the craniofacial skeleton. Results are displayed as a percentage of the initial graft volume after 1 year. The asterisks represent complete resorption of the autologous bone grafts. HA-CER, hydroxyapatite ceramic; 60% HA-CER, 60/40 hydroxyapatite/β-tricalcium phosphate; HA-CP, hydroxyapatite cement paste.
References
-
- Frommelt H. Polymers for medical applications. Macromol Chem Makromol Symp. 1987;12:281.
-
- Meekren J Van. Observationes medicochirurgicae. Amsterdam: Henrici and Bloom; 1682.
-
- Ollier L. Traite Experimental et Linique de la Regeneration des Os et de la Production Artificielle du Tissue Osseux. Paris: Masson et Fils; 1867.
-
- Macewen W. The Growth of Bone. Glasgow: J Maclehose and Sons; 1912.
-
- Barth A. Uber histologische Befunde nach Knochenimplantation. Arch Klin Chir. 1893;46:409.
LinkOut - more resources
Full Text Sources
Other Literature Sources