

Medial wall fracture: an update
- PMID: 22110807
- PMCID: PMC3052654
- DOI: 10.1055/s-0029-1224775
Medial wall fracture: an update
Abstract
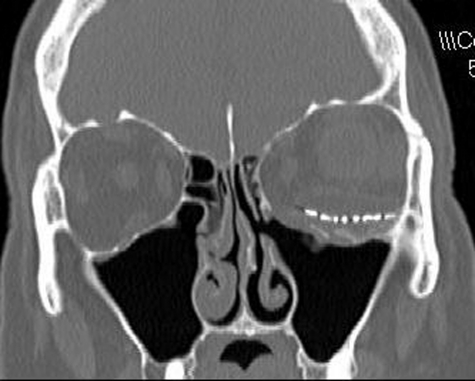
This article is a review of the literature and update for management of medial orbital wall fractures. A retrospective review of the literature was performed via PubMed to review the diagnosis and management of medial wall orbital fractures. Medial wall orbital fractures though commonly accompanying orbital floor fractures can also occur alone. There are two primary theories explaining the pathophysiology of medial wall fractures: the hydraulic theory and buckling theory. Most fractures do not require treatment. "White-eyed" trapdoor fractures necessitate immediate surgery to reduce the risk of muscle fibrosis. Trapdoor fractures are more common in the pediatric population. The vast majority of nondisplaced fractures without entrapment do not require surgery. Evaluating patients with medial wall fractures requires evaluation of muscle motility and relative enophthalmos. Patients with entrapped muscles require immediate treatment to prevent permanent injury to the muscle.
Keywords: Orbital fracture; diplopia; enophthalmos; extraocular muscle entrapment; medial wall; surgical repair.
Figures


Similar articles
-
The white-eyed medial blowout fracture.Plast Reconstr Surg. 2007 Jan;119(1):277-286. doi: 10.1097/01.prs.0000237032.59094.c2. Plast Reconstr Surg. 2007. PMID: 17255684
-
Clinical recommendations for repair of orbital facial fractures.Curr Opin Ophthalmol. 2003 Oct;14(5):236-40. doi: 10.1097/00055735-200310000-00002. Curr Opin Ophthalmol. 2003. PMID: 14502049 Review.
-
Pure orbital blowout fracture: new concepts and importance of medial orbital blowout fracture.Plast Reconstr Surg. 1999 Jun;103(7):1839-49. doi: 10.1097/00006534-199906000-00005. Plast Reconstr Surg. 1999. PMID: 10359243
-
Clinical recommendations for repair of isolated orbital floor fractures: an evidence-based analysis.Ophthalmology. 2002 Jul;109(7):1207-10; discussion 1210-1; quiz 1212-3. doi: 10.1016/s0161-6420(02)01057-6. Ophthalmology. 2002. PMID: 12093637 Review.
-
Pediatric orbital floor fracture : direct extraocular muscle involvement.Ophthalmology. 2000 Oct;107(10):1875-9. doi: 10.1016/s0161-6420(00)00334-1. Ophthalmology. 2000. PMID: 11013191
Cited by
-
Usefulness of a Transconjunctival Approach in the Reconstruction of the Medial Blow-Out Wall Fracture.Arch Craniofac Surg. 2017 Jun;18(2):76-81. doi: 10.7181/acfs.2017.18.2.76. Epub 2017 Jun 26. Arch Craniofac Surg. 2017. PMID: 28913311 Free PMC article.
-
Management of Isolated Medial Orbital Wall Fracture with Intraoral Periapical X-ray Film: A Case Report with Literature Review.J Maxillofac Oral Surg. 2024 Dec;23(6):1653-1657. doi: 10.1007/s12663-024-02315-0. Epub 2024 Aug 28. J Maxillofac Oral Surg. 2024. PMID: 39618454
-
Isolated Medial Orbital Wall Fracture Associated with Enophthalmos in a Paediatric Patient: An Unusual Presentation.Case Rep Ophthalmol. 2018 Feb 8;9(1):126-131. doi: 10.1159/000486275. eCollection 2018 Jan-Apr. Case Rep Ophthalmol. 2018. PMID: 29643794 Free PMC article.
-
Computed tomography in traumatic orbital emergencies: a pictorial essay-imaging findings, tips, and report flowchart.Insights Imaging. 2022 Jan 12;13(1):4. doi: 10.1186/s13244-021-01142-y. Insights Imaging. 2022. PMID: 35022818 Free PMC article. Review.
-
Reconstruction of Medial Orbital Wall Fractures without Subperiosteal Dissection: The "Push-Out" Technique.Arch Plast Surg. 2017 Nov;44(6):496-501. doi: 10.5999/aps.2017.01319. Epub 2017 Nov 10. Arch Plast Surg. 2017. PMID: 29121707 Free PMC article.
References
-
- Dodick J M, Galin M A, Littleton J T, Sod L M. Concomitant medial wall fracture and blowout fracture of the orbit. Arch Ophthalmol. 1971;85:273–276. - PubMed
-
- Jank S, Schuchter B, Emshoff R, et al. Clinical signs of orbital wall fractures as a function of anatomic location. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:149–153. - PubMed
-
- Rauch S D. Medial orbital blow-out fracture with entrapment. Arch Otolaryngol. 1985;111:53–55. - PubMed
-
- Thering H R, Bogart J N. Blowout fracture of the medial orbital wall, with entrapment of the medial rectus muscle. Plast Reconstr Surg. 1979;63:848–852. - PubMed
-
- Burnstine M A. Clinical recommendations for repair of orbital facial fractures. Curr Opin Ophthalmol. 2003;14:236–240. - PubMed
LinkOut - more resources
Full Text Sources