

Management of temporal bone trauma
- PMID: 22110824
- PMCID: PMC3052678
- DOI: 10.1055/s-0030-1254383
Management of temporal bone trauma
Abstract
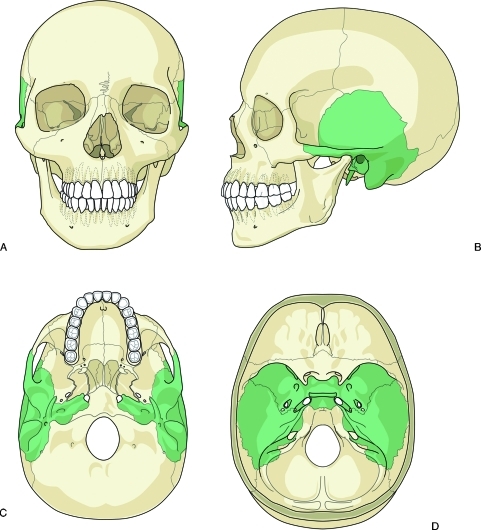
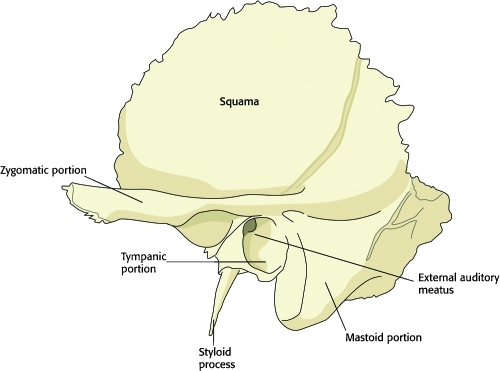
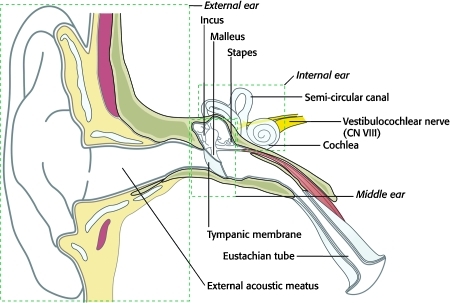
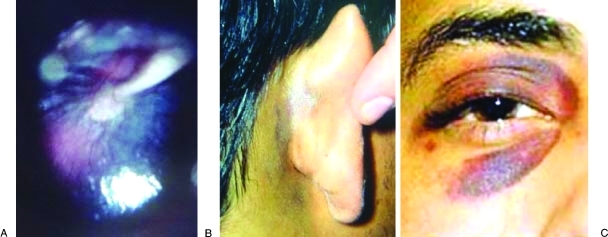
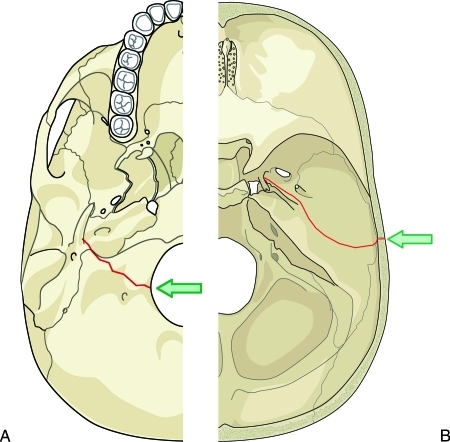
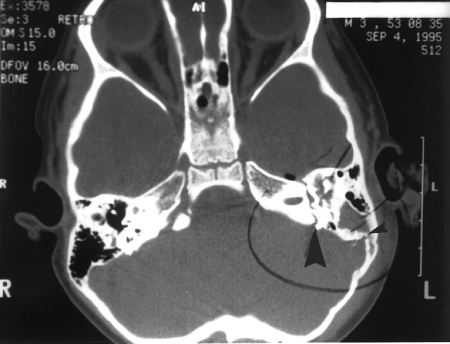
The temporal bones are paired structures located on the lateral aspects of the skull and contribute to the skull base. Trauma is usually the result of blunt head injury and can result in damage to the brain and meninges, the middle and internal ear, and the facial nerve. Complications can include intracranial hemorrhage, cerebral contusion, CSF leak and meningitis, hearing loss, vertigo, and facial paralysis. To prevent these complications, diagnosis followed by appropriate medical and surgical management is critical. Diagnosis relies primarily on physical signs and symptoms as well as radiographic imaging. Emergent intervention is required in situations involving herniation of the brain into the middle ear cavity or hemorrhage of the intratemporal carotid artery. Patients with declining facial nerve function are candidates for early surgical intervention. Conductive hearing loss can be corrected surgically as an elective procedure, while sensorineural hearing loss carries a poor prognosis, regardless of management approach. Children generally recover from temporal bone trauma with fewer complications than adults and experience a markedly lower incidence of facial nerve paralysis.
Keywords: Temporal bone; management; trauma.
Figures

References
-
- Gunlock M G, Gentry L R. Anatomy of the temporal bone. Neuroimaging Clin N Am. 1998;8(1):195–209. - PubMed
-
- Proctor B. The anatomy of the facial nerve. Otolaryngol Clin North Am. 1991;24(3):479–504. - PubMed
-
- Hasso A N, Ledington J A. Traumatic injuries of the temporal bone. Otolaryngol Clin North Am. 1988;21(2):295–316. - PubMed
-
- Wiet R J, Valvassori G E, Kotsanis C A, et al. Temporal bone fractures: state of the art review. Am J Otol. 1985;6(3):207–215. - PubMed
-
- Shindo M L, Fetterman B L, Shih L, Maceri D R, Rice D H. Gunshot wounds of the temporal bone: a rational approach to evaluation and management. Otolaryngol Head Neck Surg. 1995;112(4):533–539. - PubMed
LinkOut - more resources
Full Text Sources