

Molecular pathogenesis of endometrial and ovarian cancer
- PMID: 22112481
- PMCID: PMC3822435
- DOI: 10.3233/CBM-2011-0167
Molecular pathogenesis of endometrial and ovarian cancer
Abstract
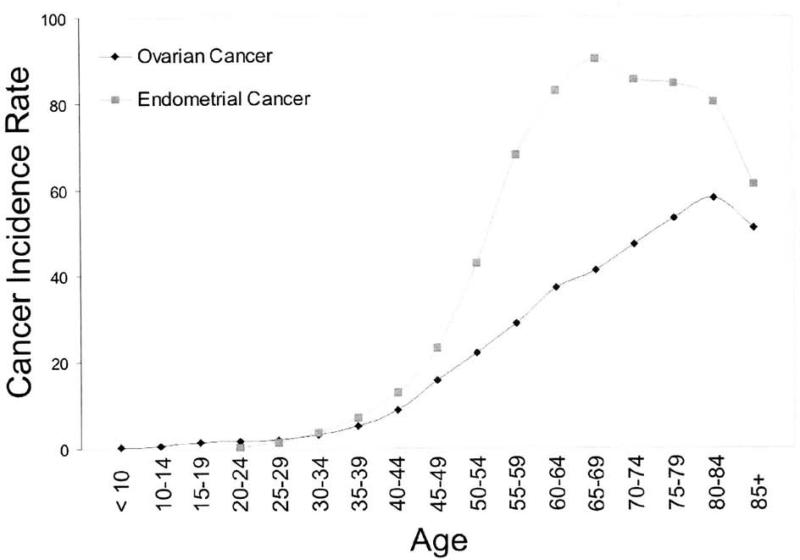
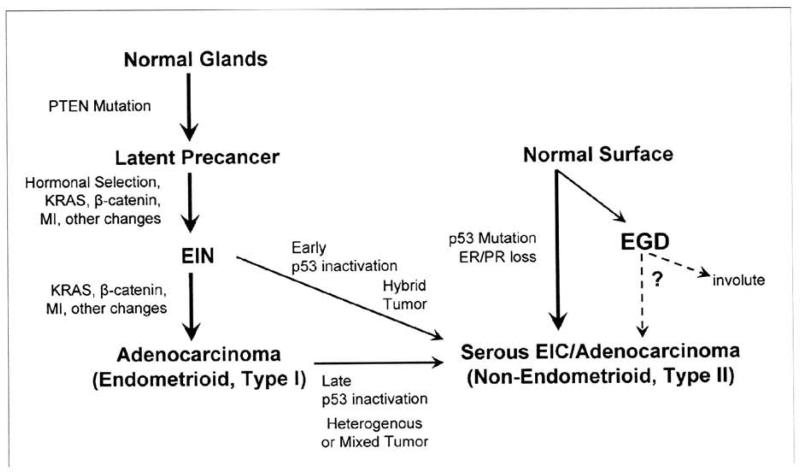
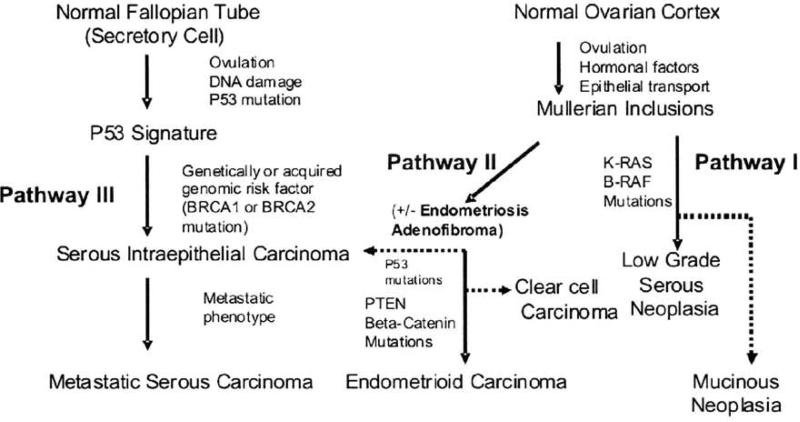
Pregnancy, breastfeeding, and oral contraceptive pill use interrupt menstrual cycles and reduce endometrial and ovarian cancer risk. This suggests the importance of turnover within Mullerian tissues, where the accumulation of mutations in p53 and PTEN has been correlated with number of cycles. The most common type of endometrial cancer (Type I) is endometrioid and molecular abnormalities include mutations in PTEN, KRAS and β-catenin. The Type I precursor is Endometrial Intraepithelial Neoplasia which displays PTEN defects. Type II endometrial cancer (whose precursors are less clear) includes serous and clear cell tumors and the most common alteration is p53 mutation. For ovarian cancer, histopathologic types parallel endometrial cancer and include serous, mucinous, endometrioid, and clear cell; some molecular features are also shared. The most frequent type of ovarian cancer is high grade serous that often displays p53 mutation and its precursor lesions may originate from normal-appearing fallopian tube epithelium that contains a p53 "signature". Mutations in KRAS, BRAF and PTEN are described in mucinous, endometrioid and low grade serous cancers and these may originate from ovarian cortical inclusion cysts. A consideration of molecular and other pathogenetic features, like epidemiology and histopathology, may provide a better understanding of endometrial and ovarian cancer.
Figures
References
-
- American Career Society Cancer Facts and Figures 2008. 2008.
-
- Parazzini F, Franceschi S, La Vecchia C, Fasoli M. The epidemiology of ovarian cancer. Gynecol Oncol. 1991;43:9–23. - PubMed
-
- Parazzini F, La Vecchia C, Bocciolone L, Franceschi S. The epidemiology of endometrial cancer. Gynecol Oncol. 1991;41:1–16. - PubMed
-
- Prentice RI, Thomson CA, Caan B, Hubbell FA, Anderson GL, Bcresford SA, Pettinger M, Lane DS, Lessin L, Yasmeen S, Singh B, Khandekar J, Shikany JM, Satterfield S, Chlebowski RT. Low-fat dietary pattern and cancer incidence in the Women's Health Initiative Dietary Modification Randomized Controlled Trial. J Natl Cancer Inst. 2007;99:1534–43. - PMC - PubMed
-
- McPherson CP, Sellers TA, Potter JD, Bostick RM, Folsom AR. Reproductive factors and risk of endometrial cancer, The Iowa Women's Health Study. Am J Epidemiol. 1996;143:1195–202. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
