

Treatment of colorectal liver metastases
- PMID: 22115124
- PMCID: PMC3251538
- DOI: 10.1186/1477-7819-9-154
Treatment of colorectal liver metastases
Abstract
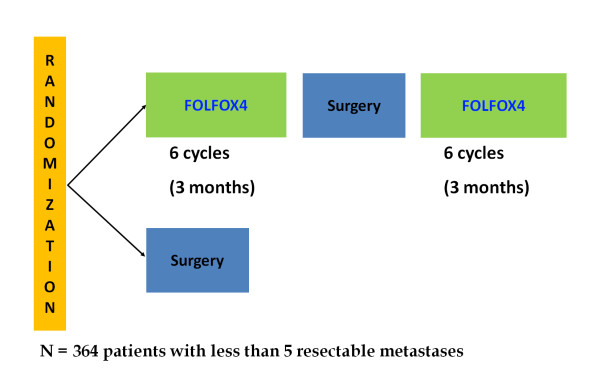
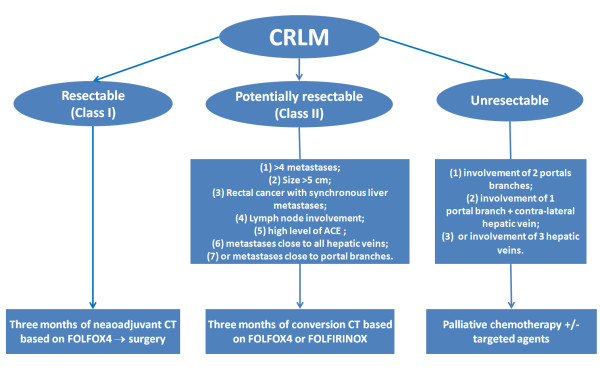
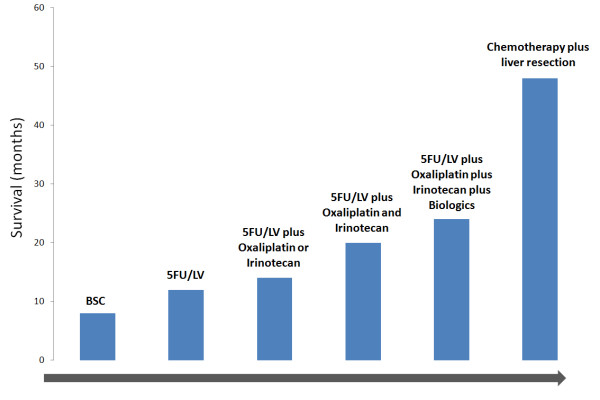
Colorectal cancer (CRC) is the third most common cancer in the word. Liver metastasis is the most common site of colorectal metastases. The prognosis of resectable colorectal liver metastases (CRLM) was improved in the recent years with the consideration of chemotherapy and surgical resection as part of the multidisciplinary management of the disease; the current 5-year survival rates after resection of liver metastases are 25% to 40%. Resectable synchronous or metachronous liver metastases should be treated with perioperative chemotherapy based on three months of FOLFOX4 (5-fluorouracil [5FU], folinic acid [LV], and oxaliplatin) chemotherapy before surgery and three months after surgery. In the case of primary surgery, pseudo-adjuvant chemotherapy for 6 months, based on 5FU/LV, FOLFOX4, XELOX (capecitabine and oxaliplatin) or FOLFIRI (5FU/LV and irinotecan), should be indicated. In potentially resectable disease, primary chemotherapy based on more intensive regimens such as FOLFIRINOX (5FU/LV, irinotecan and oxaliplatin) should be considered to enhance the chance of cure. The palliative chemotherapy based on FOLFIRI, or FOLFOX4/XELOX with or without targeted therapies, is the mainstay treatment of unresectable disease. This review would provide additional insight into the problem of optimal integration of chemotherapy and surgery in the management of CRLM.
Figures
References
-
- Adam R. Chemotherapy and surgery: new perspectives on the treatment of unresectable liver metastases. Ann Oncol. 2003;14(Suppl 2):ii13–6. - PubMed
-
- Van Cutsem E, Nordlinger B, Adam R, Köhne CH, Pozzo C, Poston G, Ychou M, Rougier P. European Colorectal Metastases Treatment Group. Towards a pan-European consensus on the treatment of patients with colorectal liver metastases. Eur J Cancer. 2006;42(14):2212–21. doi: 10.1016/j.ejca.2006.04.012. - DOI - PubMed
-
- Fong Y, Cohen AM, Fortner JG, Enker WE, Turnbull AD, Coit DG, Marrero AM, Prasad M, Blumgart LH, Brennan MF. Liver resection for colorectal metastases. J Clin Oncol. 1997;15(3):938–46. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
