

Mini-sternotomy for aortic valve replacement reduces the length of stay in the cardiac intensive care unit: meta-analysis of randomised controlled trials
- PMID: 22116090
- PMCID: PMC3225590
- DOI: 10.1136/bmjopen-2011-000266
Mini-sternotomy for aortic valve replacement reduces the length of stay in the cardiac intensive care unit: meta-analysis of randomised controlled trials
Abstract
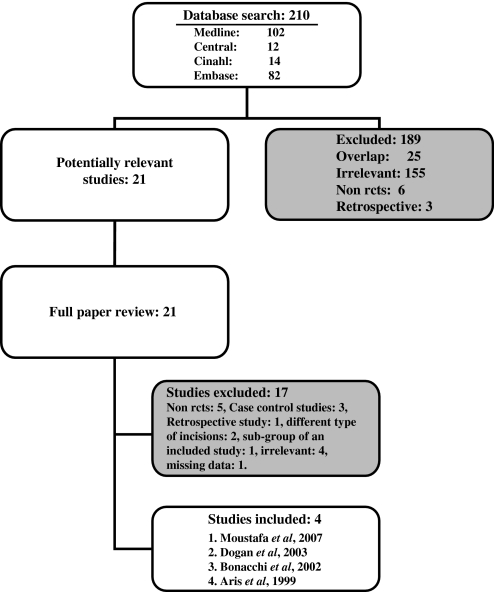
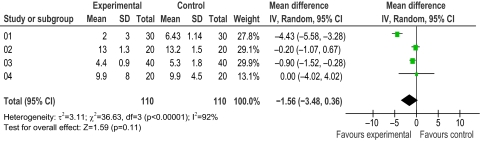
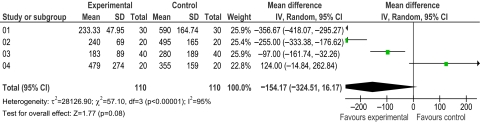
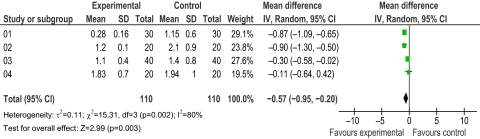
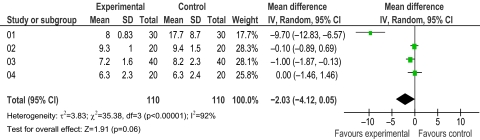
Background Mini-sternotomy for isolated aortic valve replacement aims to reduce operative trauma hastening recovery and improving the cosmetic outcome of cardiac surgery. The short-term clinical benefits from the mini-sternotomy are presumed to arise because the incision is less extensive and the lower half of the chest cage remains intact. The basic conduct of virtually all other aspects of the aortic valve replacement procedure remains the same. Therefore, similar long-term outcomes are to be expected. Objectives To conduct a meta-analysis of the only available randomised controlled trials (RCT) in the published English literature. Data sources Electronic search for relevant publications in MEDLINE, EMBASE and CENTRAL databases were performed. Four studies met the criteria. Study eligibility criteria RCT comparing minimally invasive (inverted C or L (J)-shaped) hemi-sternotomy versus conventional sternotomy for adults undergoing isolated aortic valve replacement using standard cardiopulmonary bypass technique. Methods Outcome measures were the length of positive pressure ventilation, blood loss, intensive care unit (ICU) and hospital stay. Results The length of ICU stay was significantly shorter by 0.57 days in favour of the mini-sternotomy group (CI -0.95 to -0.2; p=0.003). There was no advantage in terms of duration of ventilation (CI -3.48 to 0.36; p=0.11). However, there was some evidence to suggest a reduction in blood loss and the length of stay in hospital in the mini-sternotomy group. This did not prove to be statistically significant (154.17 ml reduction (CI -324.51 to 16.17; p=0.08) and 2.03 days less (CI -4.12 to 0.05; p=0.06), respectively). Limitations This study includes a relatively small number of subjects (n=220) and outcome variables. The risk of bias was not assessed during this meta-analysis. Conclusion Mini-sternotomy for isolated aortic valve replacement significantly reduces the length of stay in the cardiac ICU. Other short-term benefits may include a reduction in blood loss or the length of hospital stay.
Conflict of interest statement
Figures
References
-
- Brown ML, McKellar SH, Sundt TM, et al. Ministernotomy versus conventional sternotomy for aortic valve replacement: a systematic review and meta-analysis. J Thorac Cardiovasc Surg 2009;137:670–9.e5 - PubMed
-
- Murtuza B, Pepper JR, Stanbridge RD, et al. Minimal access aortic valve replacement: is it worth it? Ann Thorac Surg 2008;85:1121–31 - PubMed
-
- Moustafa MA, Abdelsamad AA, Zakaria G, et al. Minimal vs median sternotomy for aortic valve replacement. Asian Cardiovasc Thorac Ann 2007;15:472–5 - PubMed
-
- Dogan S, Dzemali O, Wimmer-Greinecker G, et al. Minimally invasive versus conventional aortic valve replacement: a prospective randomized trial. J Heart Valve Dis 2003;12:76–80 - PubMed
-
- Bonacchi M, Prifti E, Giunti G, et al. Does ministernotomy improve postoperative outcome in aortic valve operation? A prospective randomized study. Ann Thorac Surg 2002;73:460–5; discussion 465–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous