

Clinical outcome of hyperuricemia in IgA nephropathy: a retrospective cohort study and randomized controlled trial
- PMID: 22116196
- PMCID: PMC3242707
- DOI: 10.1159/000331453
Clinical outcome of hyperuricemia in IgA nephropathy: a retrospective cohort study and randomized controlled trial
Abstract
Background: Hyperuricemia is an independent risk factor for renal progression in IgA nephropathy (IgAN). However, no study has evaluated the effect of allopurinol on the clinical outcome in hyperuricemic IgAN.
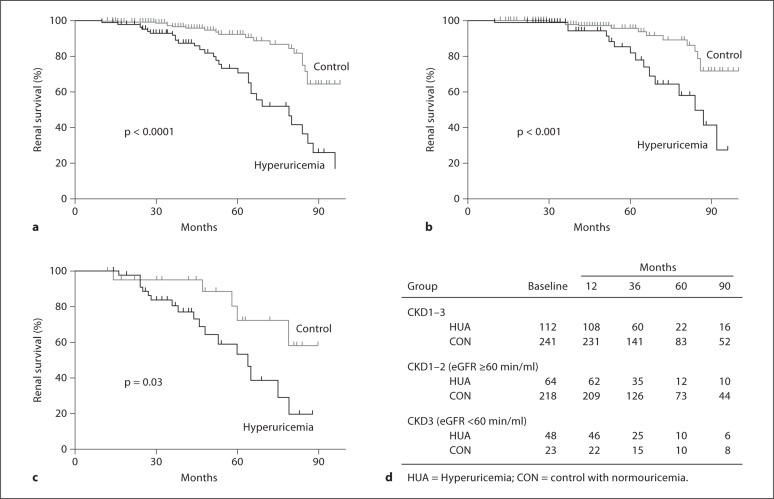
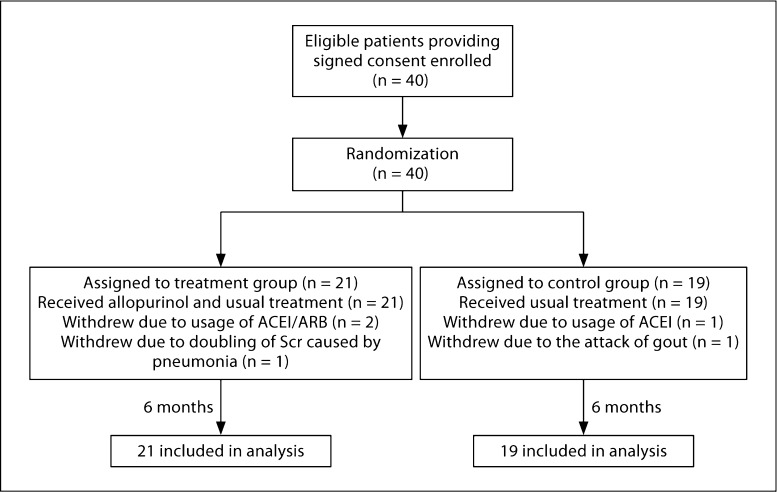
Methods: First,a retrospective cohort study of 353 IgAN patients was conducted to explore the relationship between uric acid (UA) and the progression of renal disease over a mean period of 5 years. Then, 40 hyperuricemic IgAN patients were randomized to receive allopurinol (100-300 mg/day) or usual therapy for 6 months. The study outcomes were renal disease progression and/or blood pressure.
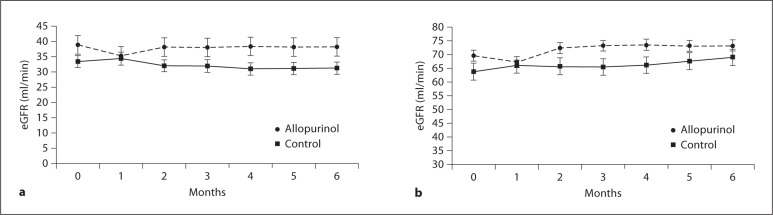
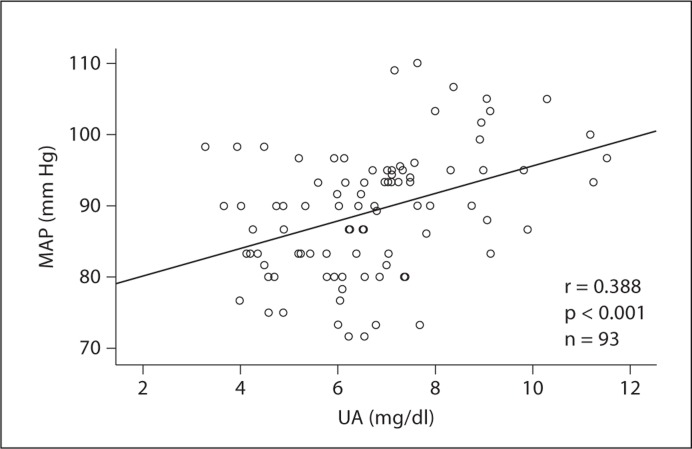
Results: Hyperuricemia independently predicted renal survival at 1, 3, and 5 years after adjustment for different baseline estimated glomerular filtration rates. In the randomized controlled trial, allopurinol did not significantly alter renal progression or proteinuria. The antihypertensive drug dosage was reduced in 7 of 9 cases with hypertension in the allopurinol group compared to 0 of 9 cases in the control group (p < 0.01). UA levels correlated with mean arterial pressure in normotensive patients (r = 0.388, p < 0.001).
Conclusion: Hyperuricemia predicts the progression of IgAN independently of baseline estimated glomerular filtration rate. Allopurinol may improve the control of blood pressure. Further studies are required to explore the effects of lowering UA on renal protection in IgAN.
Copyright © 2011 S. Karger AG, Basel.
Figures
References
-
- Radford MG, Jr, Donadio JV, Jr, Bergstralh EJ, Grande JP. Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol. 1997;8:199–207. - PubMed
-
- Syrjanen J, Mustonen J, Pasternack A. Hypertriglyceridaemia and hyperuricaemia are risk factors for progression of IgA nephropathy. Nephrol Dial Transplant. 2000;15:34–42. - PubMed
-
- Ohno I, Hosoya T, Gomi H, Ichida K, Okabe H, Hikita M. Serum uric acid and renal prognosis in patients with IgA nephropathy. Nephron. 2001;87:333–339. - PubMed
-
- Myllymaki J, Honkanen T, Syrjanen J, Helin H, Rantala I, Pasternack A, Mustonen J. Uric acid correlates with the severity of histopathological parameters in IgA nephropathy. Nephrol Dial Transplant. 2005;20:89–95. - PubMed
-
- Lee SM, Rao VM, Franklin WA, Schiffer MS, Aronson AJ, Spargo BH, Katz AI. IgA nephropathy: morphologic predictors of progressive renal disease. Hum Pathol. 1982;13:314–322. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
