

Effect of a multi-faceted quality improvement intervention on inappropriate antibiotic use in children with non-bloody diarrhoea admitted to district hospitals in Kenya
- PMID: 22117602
- PMCID: PMC3314405
- DOI: 10.1186/1471-2431-11-109
Effect of a multi-faceted quality improvement intervention on inappropriate antibiotic use in children with non-bloody diarrhoea admitted to district hospitals in Kenya
Abstract
Background: There are few reports of interventions to reduce the common but irrational use of antibiotics for acute non-bloody diarrhoea amongst hospitalised children in low-income settings. We undertook a secondary analysis of data from an intervention comprising training of health workers, facilitation, supervision and face-to-face feedback, to assess whether it reduced inappropriate use of antibiotics in children with non-bloody diarrhoea and no co-morbidities requiring antibiotics, compared to a partial intervention comprising didactic training and written feedback only. This outcome was not a pre-specified end-point of the main trial.
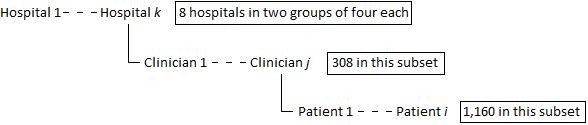
Methods: Repeated cross-sectional survey data from a cluster-randomised controlled trial of an intervention to improve management of common childhood illnesses in Kenya were used to describe the prevalence of inappropriate antibiotic use in a 7-day period in children aged 2-59 months with acute non-bloody diarrhoea. Logistic regression models with random effects for hospital were then used to identify patient and clinician level factors associated with inappropriate antibiotic use and to assess the effect of the intervention.
Results: 9, 459 admission records of children were reviewed for this outcome. Of these, 4, 232 (44.7%) were diagnosed with diarrhoea, with 130 of these being bloody (dysentery) therefore requiring antibiotics. 1, 160 children had non-bloody diarrhoea and no co-morbidities requiring antibiotics-these were the focus of the analysis. 750 (64.7%) of them received antibiotics inappropriately, 313 of these being in the intervention hospitals vs. 437 in the controls. The adjusted logistic regression model showed the baseline-adjusted odds of inappropriate antibiotic prescription to children admitted to the intervention hospitals was 0.30 times that in the control hospitals (95%CI 0.09-1.02).
Conclusion: We found some evidence that the multi-faceted, sustained intervention described in this paper led to a reduction in the inappropriate use of antibiotics in treating children with non-bloody diarrhoea.
Trial registration: International Standard Randomised Controlled Trial Number Register ISRCTN42996612.
Figures

References
-
- Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, Jha P, Campbell H, Walker CF, Cibulskis R, Eisele T, Liu L, Mathers C. Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of childhood mortality in 2008: a systematic analysis. Lancet. 2010;375:1969–1987. doi: 10.1016/S0140-6736(10)60549-1. - DOI - PubMed
-
- World Health Organisation. Pocket book of hospital care for children: guidelines for the management of common illnesses with limited resources. Geneva, Switzerland: World Health Organisation; 2005.
-
- Tawfik YM, Legros S, Geslin C. Evaluating Niger's experience in strengthening supervision, improving availability of child survival drugs though cost recovery, and initiating training for Integrated Management of Childhood Illness (IMCI) BMC Int Health Hum Rights. 2001;1:1. doi: 10.1186/1472-698X-1-1. - DOI - PMC - PubMed
-
- Pelto GH, Santos I, Goncalves H, Victoria C, Martines J, Habicht JP. Nutrition counselling training changes physician behaviour and improves caregiver knowledge acquisition. J Nutr. 2004;134:357–362. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
