

Management of acute urinary retention: a worldwide survey of 6074 men with benign prostatic hyperplasia
- PMID: 22117624
- PMCID: PMC3272343
- DOI: 10.1111/j.1464-410X.2011.10430.x
Management of acute urinary retention: a worldwide survey of 6074 men with benign prostatic hyperplasia
Abstract
Objectives: To evaluate the management of acute urinary retention (AUR) associated with benign prostatic hyperplasia (BPH) in real-life practice. To identify predictors of successful trial without catheter (TWOC).
Materials and methods: In all, 6074 men catheterized for painful AUR were enrolled in a prospective, cross-sectional survey conducted in public and private urology practices in France, Asia, Latin America, Algeria and the Middle East. Patient clinical characteristics, type of AUR and its management (type of catheterization, hospitalization, TWOC, use of α(1)-blockers, immediate or elective surgery) and adverse events observed during the catheterization period were recorded. Predictors of TWOC success were also analysed by multivariate regression analysis with stepwise procedure.
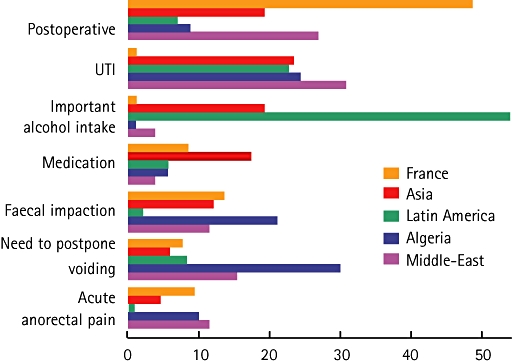
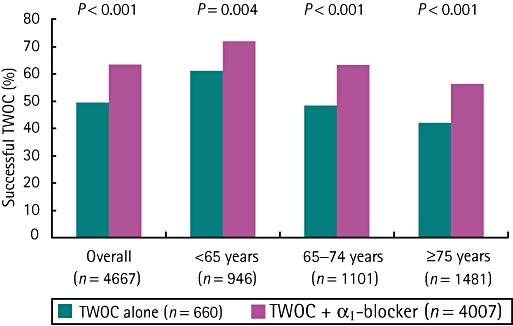
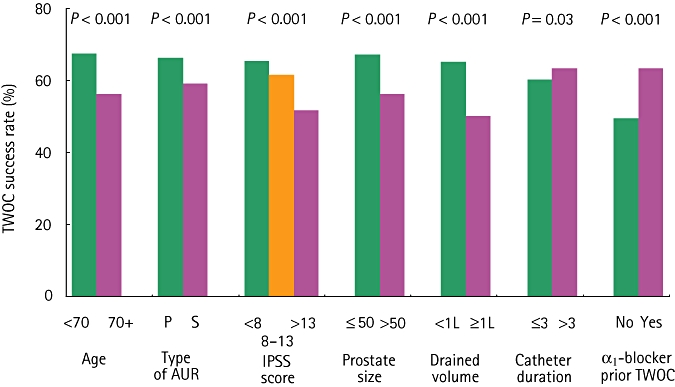
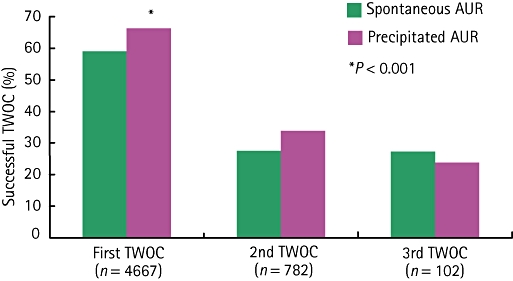
Results: Of the 6074 men, 4289 (71%) had a spontaneous AUR and 1785 (29%) had a precipitated AUR, mainly as the result of loco-regional/general anaesthesia (28.5%) and excessive alcohol intake (18.2%). Presence of BPH was revealed by AUR in 44% of men. Hospitalization for AUR varied between countries, ranging from 1.7% in Algeria to 100% in France. A urethral catheter was inserted in most cases (89.8%) usually followed by a TWOC (78.0%) after a median of 5 days. Overall TWOC success rate was 61%. Most men (86%) received an α(1)-blocker (mainly alfuzosin) before catheter removal with consistently higher TWOC success rates, regardless of age and type of AUR. Multivariate regression analysis confirmed that α(1)-blocker before TWOC doubled the chances of success (odds ratio 1.92, 95% CI 1.52-2.42, P < 0.001). Age ≥70 years, prostate size ≥50 g, severe lower urinary tract symptoms, drained volume at catheterization ≥1000 mL and spontaneous AUR favoured TWOC failure. Catheterization >3 days did not influence TWOC success but was associated with increased morbidity and prolonged hospitalization for adverse events. In the case of TWOC failure, 49% of men were recatheterized and had BPH surgery and 43.5% tried another TWOC with a success rate of 29.5%. Elective surgery was preferred to immediate surgery.
Conclusions: TWOC has become a standard practice worldwide for men with BPH and AUR. In most cases, an α(1)-blocker is prescribed before TWOC and significantly increases the chance of success. Prolonged catheterization is associated with an increased morbidity.
© 2011 THE AUTHORS. BJU INTERNATIONAL © 2011 BJU INTERNATIONAL.
Figures
References
-
- Thomas K, Oades G, Taylor-Hay C, Kirby RS. Acute urinary retention: what is the impact on quality of life? BJU Int. 2005;95:72–6. - PubMed
-
- Izard J, Nickel JC. Impact of medical therapy on transurethral resection of the prostate: two decades of change. BJU Int. 2011;108:89–93. - PubMed
-
- Jacobsen SJ, Jacobson DJ, Girman CJ, et al. Natural history of prostatism: risk factors for acute urinary retention. J Urol. 1997;158:481–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
