

The Asthma-COPD Overlap Syndrome: A Common Clinical Problem in the Elderly
- PMID: 22121384
- PMCID: PMC3205664
- DOI: 10.1155/2011/861926
The Asthma-COPD Overlap Syndrome: A Common Clinical Problem in the Elderly
Abstract
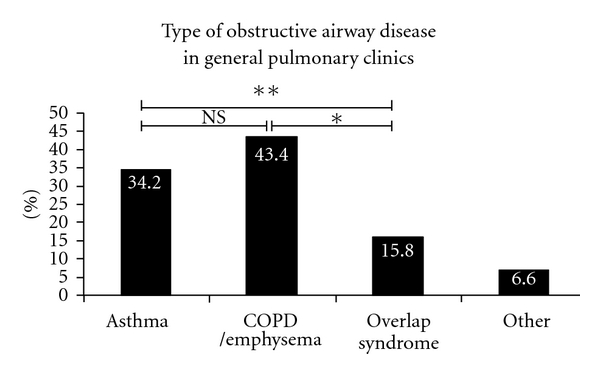
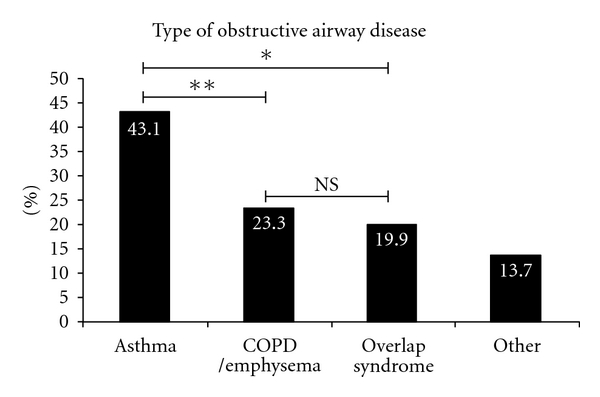
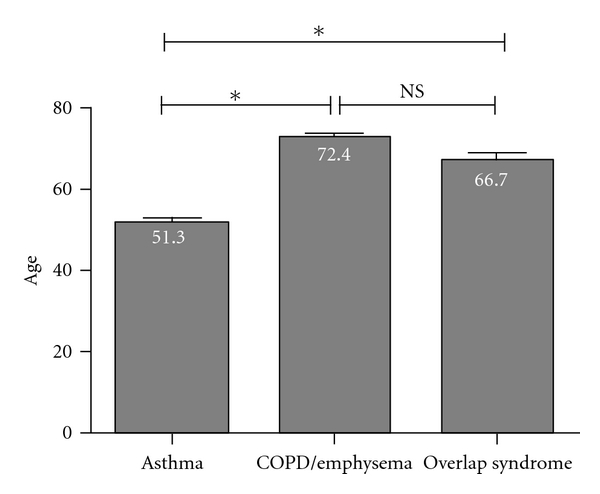
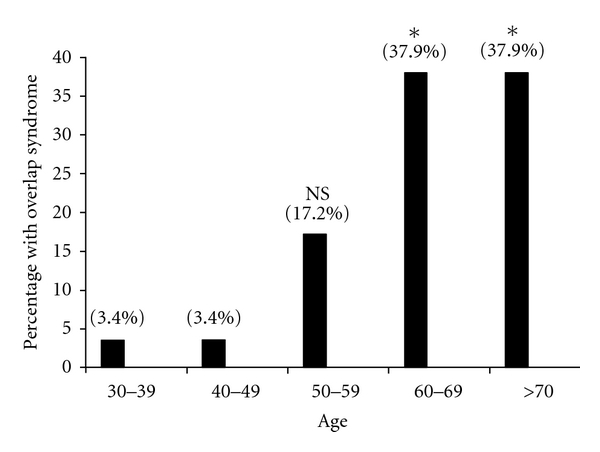
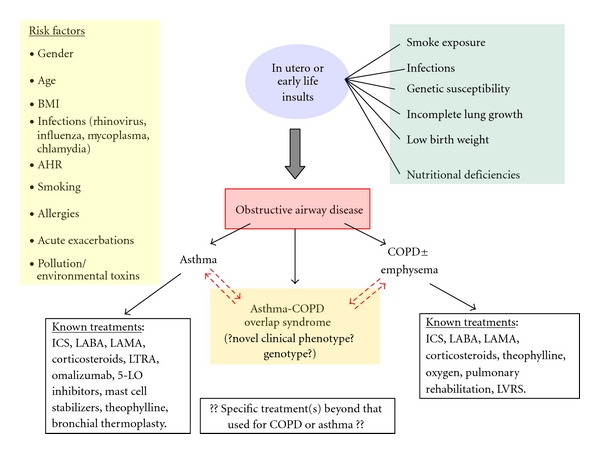
Many patients with breathlessness and chronic obstructive lung disease are diagnosed with either asthma, COPD, or-frequently-mixed disease. More commonly, patients with uncharacterized breathlessness are treated with therapies that target asthma and COPD rather than one of these diseases. This common practice represents the difficulty in distinguishing these disorders clinically, particularly in patients with a history that does not easily differentiate asthma from COPD. A common clinical scenario is an older former smoker with partially reversible or fixed airflow obstruction and evidence of atopy, demonstrating "overlap" features of asthma and COPD. We stress that asthma-COPD overlap syndrome becomes more prevalent with advancing age as patients respond less favorably to guideline-recommended drug therapy. We review the similarities and differences in clinical characteristics between these disorders, and their physiologic and inflammatory profiles within the context of the aging patient. We underscore the difficulties in differentiating asthma from COPD in current or former smokers, share our institutional experience with overlap syndrome, and highlight the need for new research to better characterize and investigate this important clinical phenotype.
Figures

References
-
- Elias J. The relationship between asthma and COPD: lessons from transgenic mice. Chest. 2004;126(2):111S–116S. - PubMed
-
- Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. American Journal of Respiratory and Critical Care Medicine. 2007;176(6):532–555. - PubMed
-
- Shaya FT, Dongyi D, Akazawa MO, et al. Burden of concomitant asthma and COPD in a Medicaid population. Chest. 2008;134(1):14–19. - PubMed
-
- Celli BR, MacNee W, Agusti A, et al. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. European Respiratory Journal. 2004;23(6):932–946. - PubMed
-
- Mannino DM. Coexisting Asthma and COPD: confused clinicians or poor prognosticator? Chest. 2008;134(1):1–2. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
