

Coeliac plexus block in the management of chronic abdominal pain due to severe diabetic gastroparesis
- PMID: 22121392
- PMCID: PMC3027778
- DOI: 10.1136/bcr.06.2009.1986
Coeliac plexus block in the management of chronic abdominal pain due to severe diabetic gastroparesis
Abstract
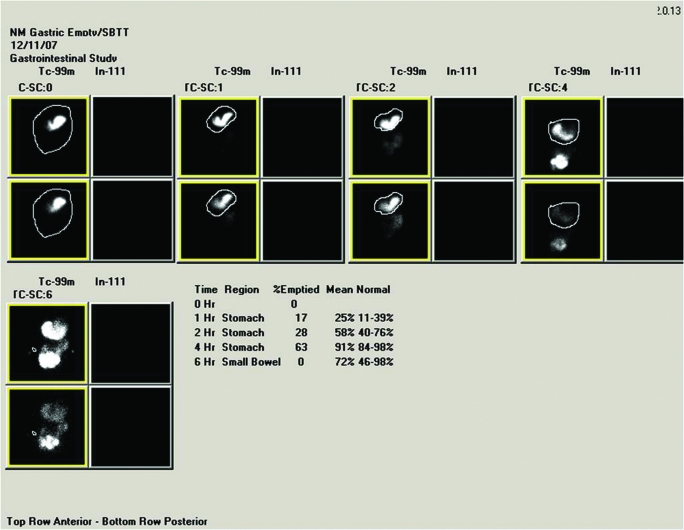
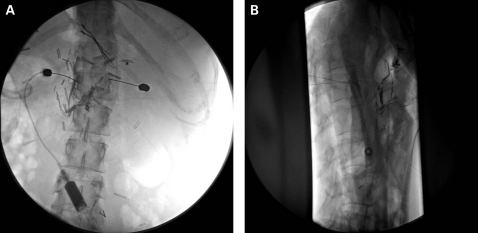
Abdominal pain can be disabling in patients with gastroparesis. The pathogenesis of pain in these individuals is poorly understood. Agents commonly used in clinical practice, including tricyclic antidepressants, gabapentin, and pregabalin, have remained largely unsatisfactory in treating this pain. We report the case of a 50-year-old woman presenting with chronic unrelenting abdominal pain due to severe diabetic gastroparesis that was managed successfully with coeliac plexus block with local anaesthesia and steroid injection. Adequate analgesia was achieved and maintained for 10 weeks following the coeliac plexus block, which allowed elimination of opiate requirements for pain management (and avoidance of narcotic associated constipation), continuation of percutaneous endoscopy jejunostomy tube feedings, and avoidance of long term parenteral nutrition.
Figures
Similar articles
-
[The anterior sonographic-guided celiac plexus blockade. Review and personal observations].Anaesthesist. 1993 Apr;42(4):246-55. Anaesthesist. 1993. PMID: 8488998 Review. German.
-
Breaking the pain cycle successfully in a child with severe pain due to recurrent pancreatitis: A case report.J Pak Med Assoc. 2021 Sep;71(9):2268-2270. doi: 10.47391/JPMA.302. J Pak Med Assoc. 2021. PMID: 34580529
-
Clinical trial: a randomized trial comparing fluoroscopy guided percutaneous technique vs. endoscopic ultrasound guided technique of coeliac plexus block for treatment of pain in chronic pancreatitis.Aliment Pharmacol Ther. 2009 May 1;29(9):979-84. doi: 10.1111/j.1365-2036.2009.03963.x. Aliment Pharmacol Ther. 2009. PMID: 19222416 Clinical Trial.
-
Palliation by coeliac plexus block for upper abdominal visceral cancer pain.Trop Doct. 2002 Oct;32(4):224-6. doi: 10.1177/004947550203200413. Trop Doct. 2002. PMID: 12405303 Clinical Trial.
-
[Coeliac plexus block in patients with pancreatic tumour pain].Ned Tijdschr Geneeskd. 2006 Apr 1;150(13):723-8. Ned Tijdschr Geneeskd. 2006. PMID: 16623345 Review. Dutch.
Cited by
-
Treatment of patients with diabetic gastroparesis.Gastroenterol Hepatol (N Y). 2010 Jun;6(6):1-16. Gastroenterol Hepatol (N Y). 2010. PMID: 20733935 Free PMC article.
-
Current Concepts in Gastroparesis and Gastric Neuromuscular Disorders-Pathophysiology, Diagnosis, and Management.Diagnostics (Basel). 2025 Apr 5;15(7):935. doi: 10.3390/diagnostics15070935. Diagnostics (Basel). 2025. PMID: 40218285 Free PMC article. Review.
-
Celiac plexus block in the management of chronic abdominal pain.Curr Pain Headache Rep. 2014 Feb;18(2):394. doi: 10.1007/s11916-013-0394-z. Curr Pain Headache Rep. 2014. PMID: 24414338 Review.
-
Chronic abdominal pain secondary to mesenteric panniculitis treated successfully with endoscopic ultrasonography-guided celiac plexus block: A case report.World J Gastrointest Endosc. 2015 May 16;7(5):563-6. doi: 10.4253/wjge.v7.i5.563. World J Gastrointest Endosc. 2015. PMID: 25992196 Free PMC article.
-
Treatment of refractory diabetic gastroparesis: Western medicine and traditional Chinese medicine therapies.World J Gastroenterol. 2014 Jun 7;20(21):6504-14. doi: 10.3748/wjg.v20.i21.6504. World J Gastroenterol. 2014. PMID: 24914371 Free PMC article. Review.
References
-
- He CL, Soffer EE, Ferris CD, et al. Loss of interstitial cells of Cajal and inhibitory innervation in insulin-dependent diabetes. Gastroenterology 2001; 121: 427–34 - PubMed
-
- Hoogerwerf WA, Pasricha PJ, Kalloo AN, et al. Pain: the overlooked symptom in gastroparesis. Am J Gastroenterol 1999; 94: 1029–33 - PubMed
-
- Camilleri M. Diabetic Gastroparesis. N Engl J Med 2007; 356: 820–9 - PubMed
LinkOut - more resources
Full Text Sources