

Conservative treatment of idiopathic scoliosis according to FITS concept: presentation of the method and preliminary, short term radiological and clinical results based on SOSORT and SRS criteria
- PMID: 22122964
- PMCID: PMC3286410
- DOI: 10.1186/1748-7161-6-25
Conservative treatment of idiopathic scoliosis according to FITS concept: presentation of the method and preliminary, short term radiological and clinical results based on SOSORT and SRS criteria
Abstract
Background: Conservative scoliosis therapy according to the FITS Concept is applied as a unique treatment or in combination with corrective bracing. The aim of the study was to present author's method of diagnosis and therapy for idiopathic scoliosis FITS-Functional Individual Therapy of Scoliosis and to analyze the early results of FITS therapy in a series of consecutive patients.
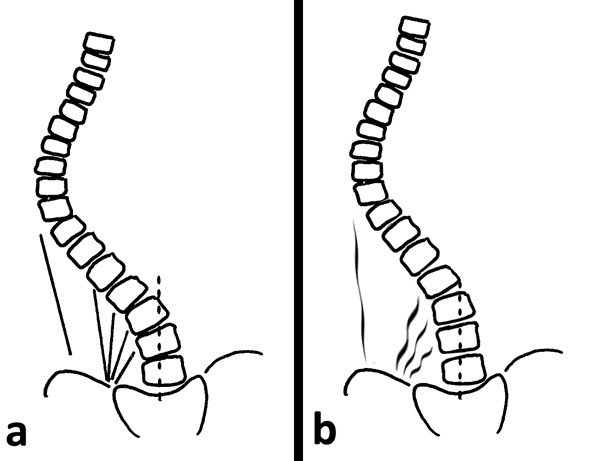
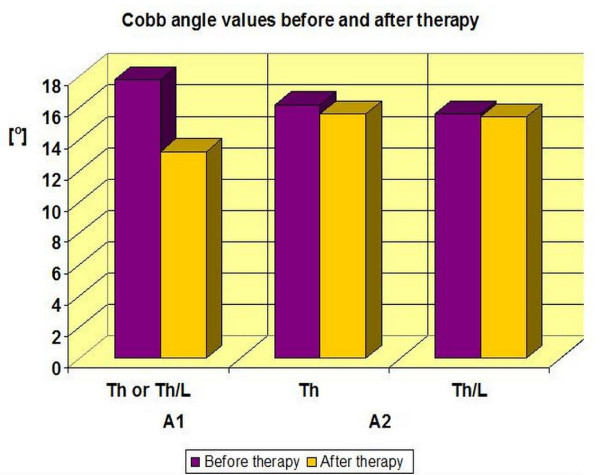
Methods: The analysis comprised separately: (1) single structural thoracic, thoracolumbar or lumbar curves and (2) double structural scoliosis-thoracic and thoracolumbar or lumbar curves. The Cobb angle and Risser sign were analyzed at the initial stage and at the 2.8-year follow-up. The percentage of patients improved (defined as decrease of Cobb angle of more than 5 degrees), stable (+/- 5 degrees), and progressed (increase of Cobb angle of more than 5 degrees) was calculated. The clinical assessment comprised: the Angle of Trunk Rotation (ATR) initial and follow-up value, the plumb line imbalance, the scapulae level and the distance from the apical spinous process of the primary curve to the plumb line.
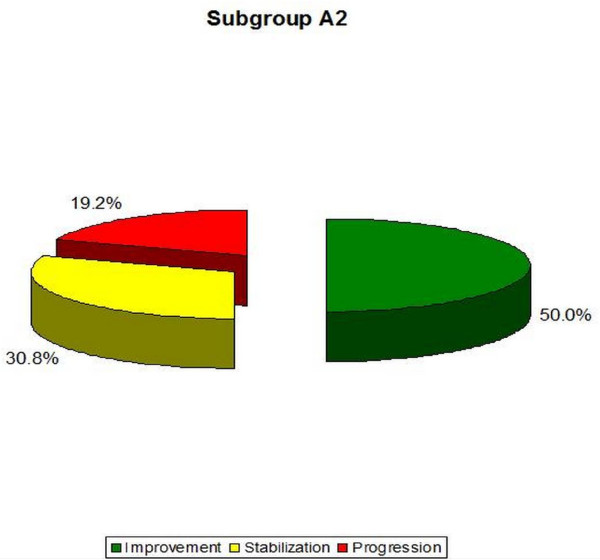
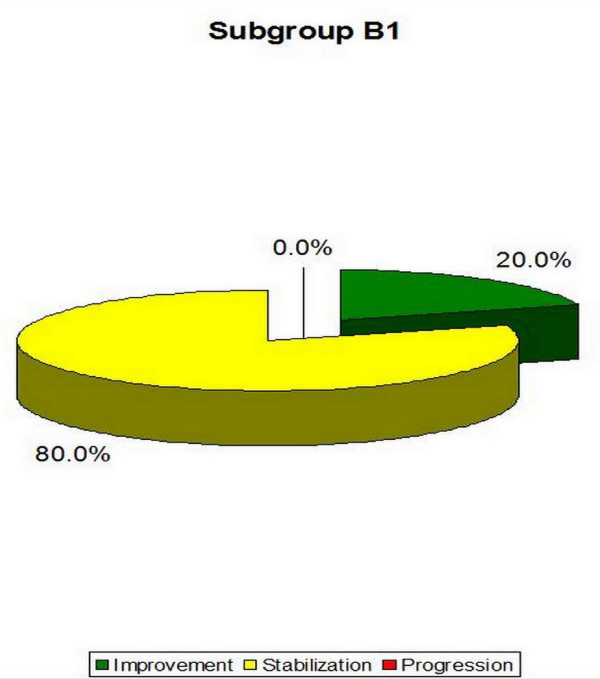
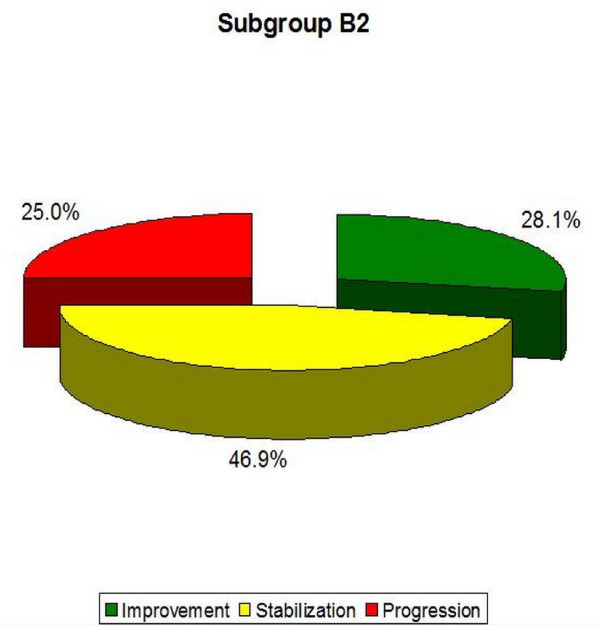
Results: In the Group A: (1) in single structural scoliosis 50,0% of patients improved, 46,2% were stable and 3,8% progressed, while (2) in double scoliosis 50,0% of patients improved, 30,8% were stable and 19,2% progressed. In the Group B: (1) in single scoliosis 20,0% of patients improved, 80,0% were stable, no patient progressed, while (2) in double scoliosis 28,1% of patients improved, 46,9% were stable and 25,0% progressed.
Conclusion: Best results were obtained in 10-25 degrees scoliosis which is a good indication to start therapy before more structural changes within the spine establish.
Figures




























References
-
- Rigo M, Reiter C, Weiss HR. Effect of conservative management on the prevalence of surgery in patients with adolescent idiopathic scoliosis. Pediatr Rehabil. 2003;6(3-4):209–214. - PubMed
-
- Maruyama T, Kitagawa T, Takeshita K, Mochizuki K, Nakamura K. Conservative treatment for adolescent idiopathic scoliosis: can it reduce the incidence of surgical treatment? Pediatr Rehabil. 2003;6(3-4):215–219. - PubMed
-
- Negrini S, Atanasio S, Zaina F, Romano M, Parzini S, Negrini A. End-growth results of bracing and exercises for adolescent idiopathic scoliosis. Prospective worst-case analysis. Stud Health Technol Inform. 2008;135:395–408. - PubMed
-
- Negrini S, Negrini A, Romano M, Verzini N, Parzini S. A controlled prospective study on the efficacy of SEAS.02 exercises in preparation to bracing for idiopathic scoliosis. Stud Health Technol Inform. 2006;123:519–522. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
