

Improving care after myocardial infarction using a 2-year internet-delivered intervention: the Department of Veterans Affairs myocardial infarction-plus cluster-randomized trial
- PMID: 22123798
- PMCID: PMC6521717
- DOI: 10.1001/archinternmed.2011.498
Improving care after myocardial infarction using a 2-year internet-delivered intervention: the Department of Veterans Affairs myocardial infarction-plus cluster-randomized trial
Abstract
Background: Cardiovascular risk reduction in ambulatory patients who survive myocardial infarction (MI) is effective but underused. We sought to evaluate a provider-directed, Internet-delivered intervention to improve cardiovascular management for post-MI outpatients.
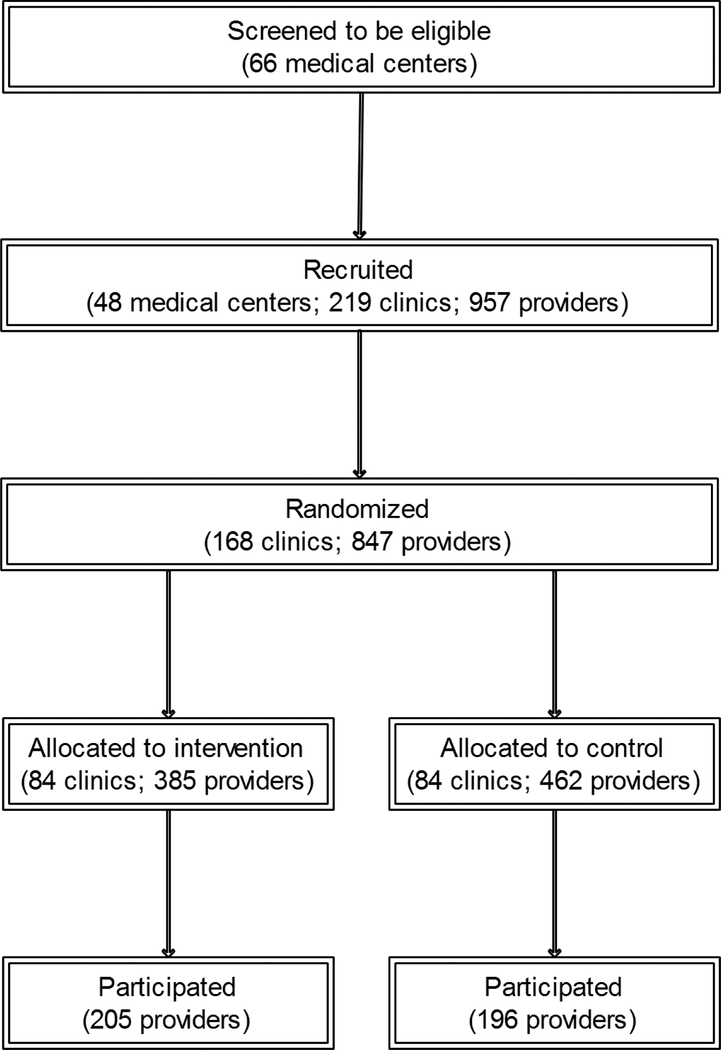
Methods: The Department of Veterans Affairs (VA) MI-Plus study was a cluster-randomized trial involving 168 community-based primary care clinics and 847 providers in 26 states, the Virgin Islands, and Puerto Rico, from January 1, 2002, through December 31, 2008, with the clinic as the randomization unit. We collected administrative data for 15,847 post-MI patients and medical record data for 10,452 of these. A multicomponent, Internet-delivered intervention included quarterly educational modules, practice guidelines, monthly literature summaries, and automated e-mail reminders delivered to providers for 27 months. Main outcome measures included percentage of patients who achieved each of 7 clinical indicators, a composite score of the 7 clinical indicators, and mean low-density lipoprotein cholesterol and hemoglobin A(1c) levels.
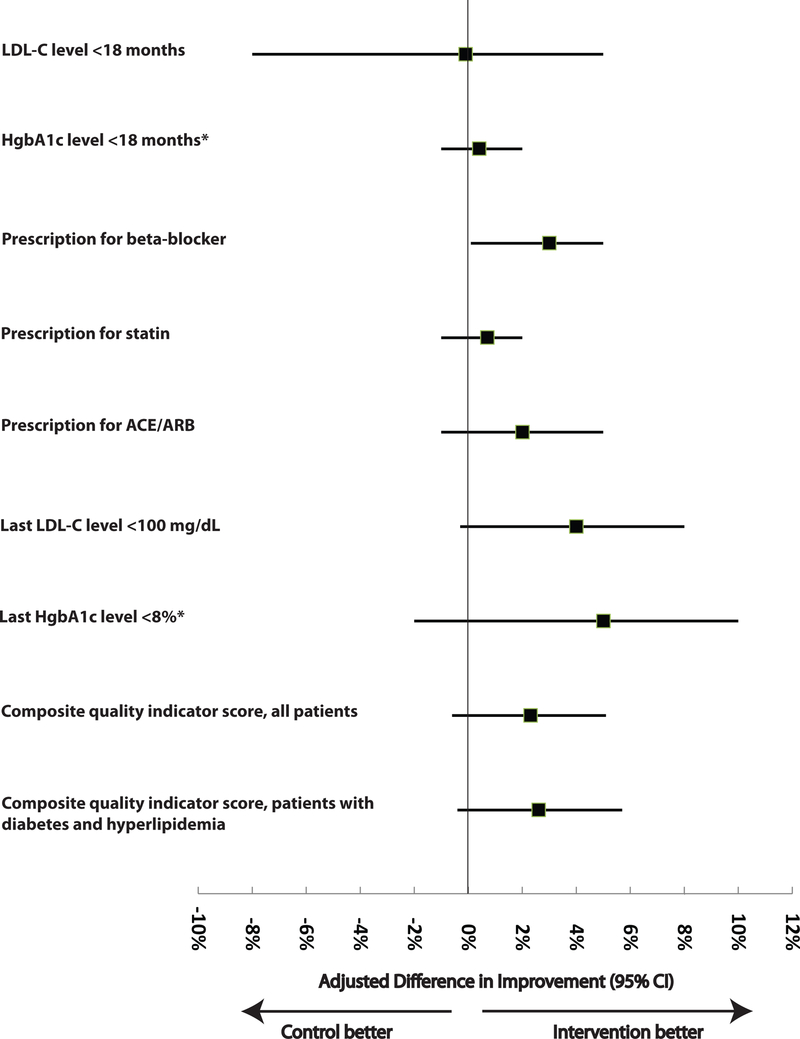
Results: Clinics had a median of 3 providers (interquartile range, 2-6), with a median of 50.0% of providers (33.3%-66.7%) participating in the study. Patients in intervention clinics had greater improvements (from 70.0% to 85.5%) in the percentages prescribed β-blockers than patients in control clinics (71.9% to 84.0%; adjusted improvement gain for intervention vs control, 2.6%; 95% CI, 0.1%-4.1%). We found nonsignificant differences in improvements favoring patients in intervention clinics for 5 of 6 remaining clinical indicators and levels of low-density lipoprotein cholesterol and hemoglobin A(1c).
Conclusion: A longitudinal, Internet-delivered intervention improved only 1 of 7 clinical indicators of cardiovascular management in ambulatory post-MI patients.
Figures
Comment in
-
Being successful at prevention: making it easy to do the right thing: comment on "Improving care after myocardial infarction using a 2-year internet-delivered intervention".Arch Intern Med. 2011 Nov 28;171(21):1917-9. doi: 10.1001/archinternmed.2011.532. Arch Intern Med. 2011. PMID: 22123799 No abstract available.
References
-
- Flather MD, Yusuf S, Kober L, et al. Long-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: a systematic overview of data from individual patients. ACE-Inhibitor Myocardial Infarction Collaborative Group. Lancet. 2000;355(9215):1575–1581. - PubMed
-
- Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366(9493):1267–1278. - PubMed
