

Distinguishing persistent insulin autoantibodies with differential risk: nonradioactive bivalent proinsulin/insulin autoantibody assay
- PMID: 22124462
- PMCID: PMC3237666
- DOI: 10.2337/db11-0670
Distinguishing persistent insulin autoantibodies with differential risk: nonradioactive bivalent proinsulin/insulin autoantibody assay
Abstract
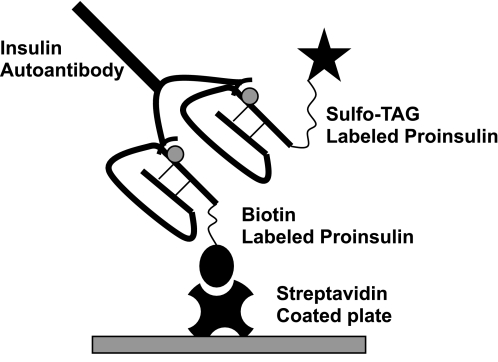
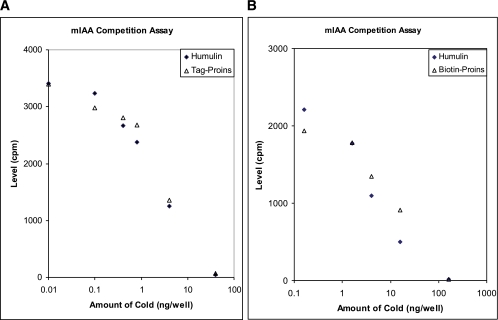
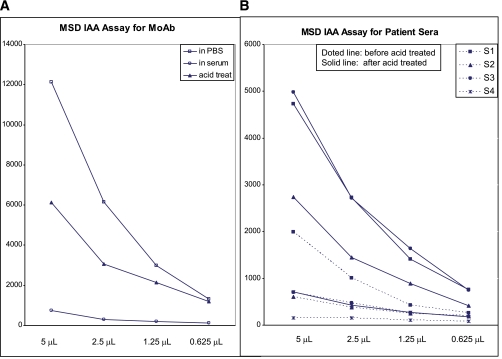
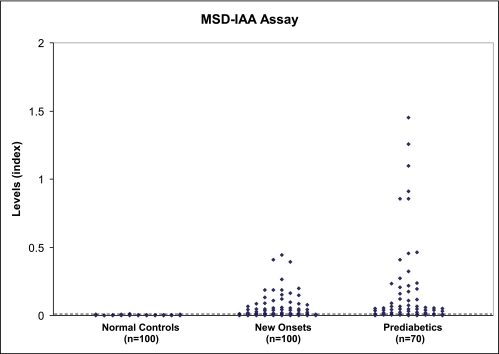
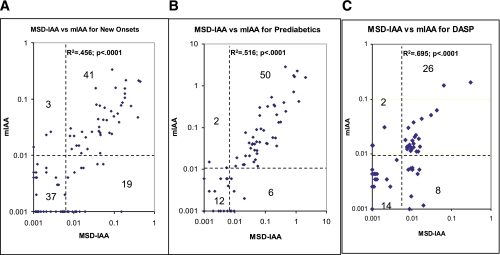
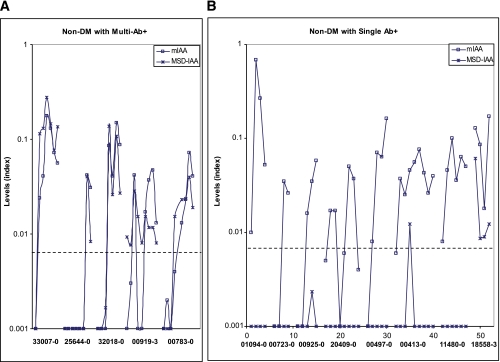
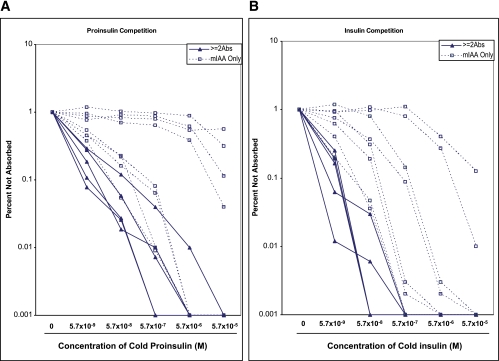
A subset of children develops persistent insulin autoantibodies (IAA; almost always as the only islet autoantibody) without evidence of progression to diabetes. The aim of the current study was the development and characterization of the performance of a nonradioactive fluid phase IAA assay in relation to standard IAA radioassay. We developed a nonradioactive IAA assay where bivalent IAA cross-link two insulin moieties in a fluid phase. The serum samples positive for anti-islet autoantibodies from 150 newly diagnosed patients with diabetes (Barbara Davis Center plus Diabetes Autoantibody Standardization Program [DASP] workshop) and 70 prediabetic subjects who were followed to diabetes were studied. In addition, sequential samples from 64 nondiabetic subjects who were persistently IAA(+) were analyzed. With 99th percentile of specificity, the new assay with the technology from Meso Scale Discovery Company (MSD-IAA) detects as positive 61% (61 of 100) of new-onset patients and 80% (56 of 70) of prediabetic patients compared with our current fluid phase micro-IAA radioassay (mIAA; 44 and 74%, respectively). In addition, MSD-IAA demonstrated better sensitivity than our mIAA from blinded DASP workshop (68 vs. 56% with the same 99% specificity). Of 64 IAA(+) nondiabetic subjects, 25% (8 of 32) who had only IAA and thus the low risk for progression to diabetes were positive with MSD-IAA assay. In contrast, 100% (32 of 32) high-risk children (IAA plus other islet autoantibodies) were positive with MSD-IAA. The IAA detectable by radioassay, but not MSD-IAA, were usually of lower affinity compared with the IAA of the high-risk children. These data suggest that a subset of IAA with current radioassay (not MSD-IAA) represents biologic false positives in terms of autoimmunity leading to diabetes. We hypothesize that factors related to the mechanism of loss of tolerance leading to diabetes determine high affinity and MSD-IAA reactivity.
Figures
References
-
- Williams AJK, Bingley PJ, Bonifacio E, Palmer JP, Gale EAM. A novel micro-assay for insulin autoantibodies. J Autoimmun 1997;10:473–478 - PubMed
-
- Törn C, Mueller PW, Schlosser M, Bonifacio E, Bingley PJ; Participating Laboratories Diabetes Antibody Standardization Program: evaluation of assays for autoantibodies to glutamic acid decarboxylase and islet antigen-2. Diabetologia 2008;51:846–852 - PubMed
-
- Greenbaum CJ, Palmer JP, Kuglin B, Kolb H. Insulin autoantibodies measured by radioimmunoassay methodology are more related to insulin-dependent diabetes mellitus than those measured by enzyme-linked immunosorbent assay: results of the Fourth International Workshop on the Standardization of Insulin Autoantibody Measurement. J Clin Endocrinol Metab 1992;74:1040–1044 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
