

The accommodative lag of the young hyperopic patient
- PMID: 22125280
- PMCID: PMC3292355
- DOI: 10.1167/iovs.11-8174
The accommodative lag of the young hyperopic patient
Abstract
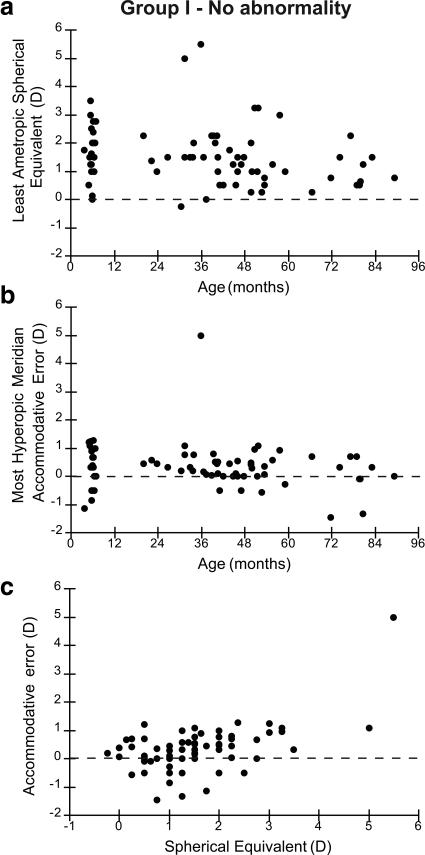
Purpose: To determine the accommodative accuracy of infants and young children before they had had any form of clinical intervention or treatment, in an attempt to determine the difference between 'normal' and 'abnormal' visual experience for these individuals.
Methods: Nott retinoscopy was performed on 111 subjects in binocular viewing conditions at a viewing distance of 50 cm. The target was a naturalistic cartoon image with a broadband spatial frequency amplitude spectrum.
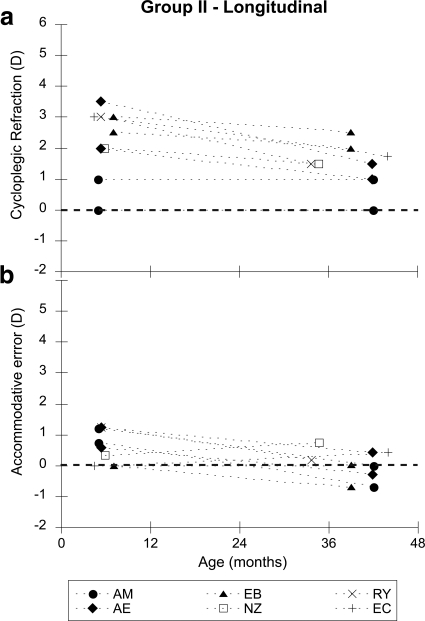
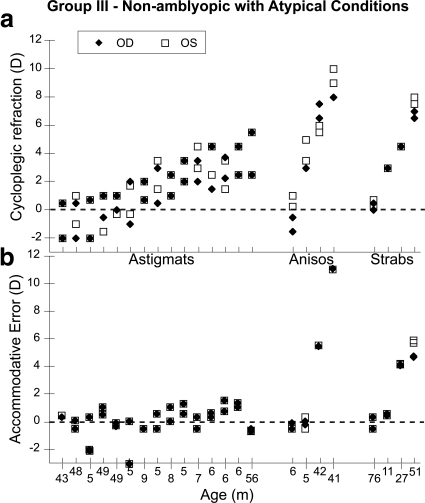
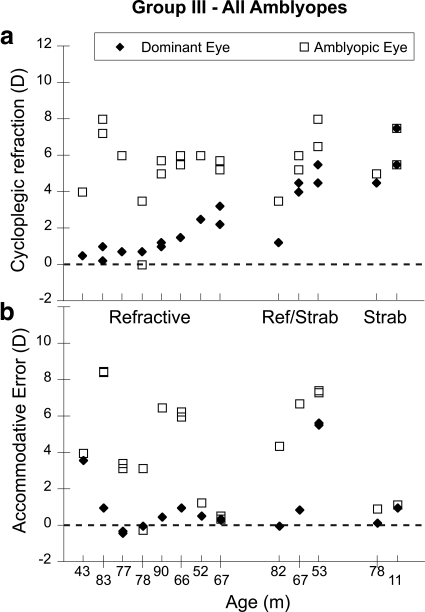
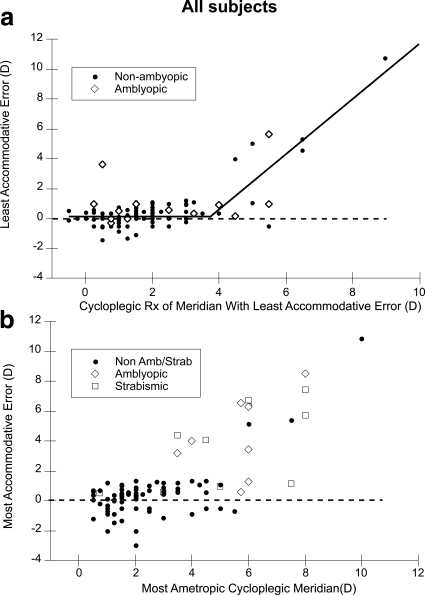
Results: Accommodative accuracy was not related to age (4-90 months). In the group found to have no apparent clinical abnormality (n = 71), the mean lag in the more hyperopic meridian of the least ametropic eye was 0.34 diopters (D). When considering the group as a whole, those with less than approximately 4 D of hyperopia demonstrated similar lags, while those with higher hyperopia, amblyopia, or strabismus had more variable lags. An ROC analysis designed to detect hyperopia >5 D in any meridian, amblyopia and/or strabismus had an area under the curve of 0.90 (95% confidence interval [CI], 0.82 to 0.95), and for a lag criterion of 1.3 D had a sensitivity of 83.3% and a specificity of 96.5%.
Conclusions: These data from a relatively small but broad sampling of age and clinical status suggest that clinically normal young infants and children with low amounts of hyperopia have similar lags of accommodation from the first few months after birth. Subjects with greater than 4 D of hyperopia, or amblyopia or strabismus, have more variable lags and therefore evidence of abnormal visual experience.
Figures
References
-
- Mitchell DE, Timney B. Postnatal development of function in the mammalian visual system. In: Kandel ER, ed. Handbook of Physiology. The Nervous System III. Vol. 3 Washington DC: American Physiological Society; 1984:507–555
-
- Troilo D. Neonatal eye growth and emmetropisation–a literature review. Eye. 1992;6:154–160 - PubMed
-
- Smith EI. Environmentally induced refractive errors in animals. In: Rosenfield M, Gilmartin B, eds. Myopia and Nearwork. Oxford: Butterworth-Heinemann; 1998:57–90
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
