

How genetically heterogeneous is Kabuki syndrome?: MLL2 testing in 116 patients, review and analyses of mutation and phenotypic spectrum
- PMID: 22126750
- PMCID: PMC3306863
- DOI: 10.1038/ejhg.2011.220
How genetically heterogeneous is Kabuki syndrome?: MLL2 testing in 116 patients, review and analyses of mutation and phenotypic spectrum
Abstract
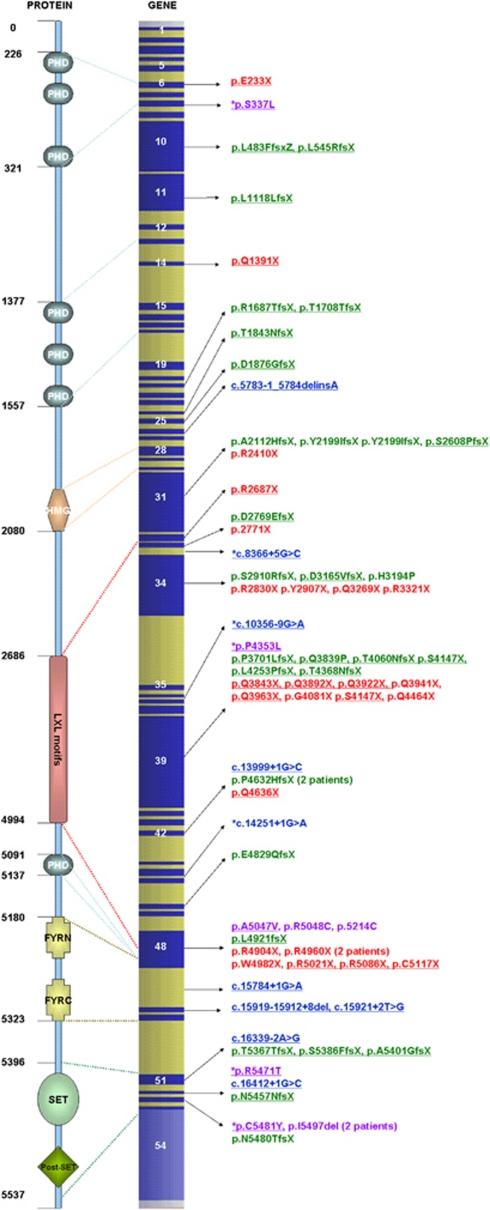
MLL2 mutations are detected in 55 to 80% of patients with Kabuki syndrome (KS). In 20 to 45% patients with KS, the genetic basis remains unknown, suggesting possible genetic heterogeneity. Here, we present the largest yet reported cohort of 116 patients with KS. We identified MLL2 variants in 74 patients, of which 47 are novel and a majority are truncating. We show that pathogenic missense mutations were commonly located in exon 48. We undertook a systematic facial KS morphology study of patients with KS at our regional dysmorphology meeting. Our data suggest that nearly all patients with typical KS facial features have pathogenic MLL2 mutations, although KS can be phenotypically variable. Furthermore, we show that MLL2 mutation-positive KS patients are more likely to have feeding problems, kidney anomalies, early breast bud development, joint dislocations and palatal malformations in comparison with MLL2 mutation-negative patients. Our work expands the mutation spectrum of MLL2 that may help in better understanding of this molecule, which is important in gene expression, epigenetic control of active chromatin states, embryonic development and cancer. Our analyses of the phenotype indicates that MLL2 mutation-positive and -negative patients differ systematically, and genetic heterogeneity of KS is not as extensive as previously suggested. Moreover, phenotypic variability of KS suggests that MLL2 testing should be considered even in atypical patients.
Figures


References
-
- Kuroki Y, Suzuki Y, Chyo H, Hata A, Matsui I. A new malformation syndrome of long palpebralfissures, large ears, depressed nasal tip, and skeletal anomalies associated with postnatal dwarfism and mental retardation. J Pediatr. 1981;99:570–573. - PubMed
-
- Niikawa N, Matsuura N, Fukushima Y, Ohsawa T, Kajii T. Kabuki make-up syndrome: a syndrome of mental retardation, unusual facies, large and protruding ears, and postnatal growth deficiency. J Pediatr. 1981;99:565–569. - PubMed
-
- Adam MP, Hudgins L. Kabuki syndrome: a review. Clin Genet. 2005;67:209–219. - PubMed
-
- Paulussen ADC, Stegmann APA, Blok MJ, et al. MLL2 mutation spectrum in 45 patients with Kabuki syndrome. Hum Mutat. 2011;32:E2018–E2025. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
