

A randomized trial of long-term remote monitoring of pacemaker recipients (the COMPAS trial)
- PMID: 22127418
- PMCID: PMC3341630
- DOI: 10.1093/eurheartj/ehr419
A randomized trial of long-term remote monitoring of pacemaker recipients (the COMPAS trial)
Abstract
Aims: Professional practice guidelines recommend that pacemaker recipients be followed regularly. However, the majority of scheduled ambulatory visits is unproductive and imposes a heavy burden on the health-care system.
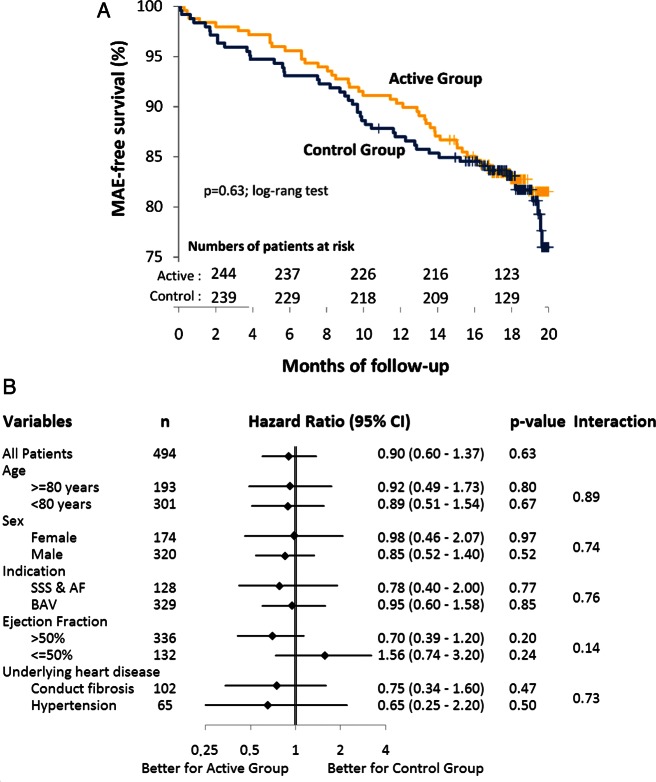
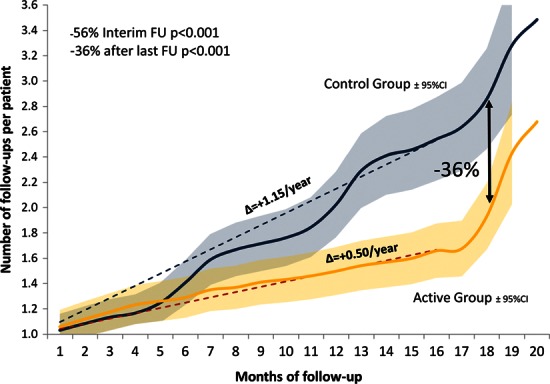
Methods and results: The COMPAS randomized, multicentre, non-inferiority trial examined the safety of long-term remote monitoring of pacemakers. Between December 2005 and January 2008, 538 patients were randomly assigned to remote monitoring follow-up (active group) vs. standard care (control group). The primary objective was to confirm that the proportion of patients who experienced at least one major adverse event (MAE), including all-cause death and hospitalizations for device-related or cardiovascular adverse events, was not >7% higher in the active than in the control group. MAE-free survivals and quality of life were compared in both groups. The characteristics of the study groups were similar. Over a follow-up of 18.3 months, 17.3% of patients in the active and 19.1% in the control group experienced at least one MAE (P < 0.01 for non-inferiority). Hospitalizations for atrial arrhythmias (6 vs. 18) and strokes (2 vs. 8) were fewer (P < 0.05), and the number of interim ambulatory visits was 56% lower (P < 0.001) in the active than the control group. Changes in pacemaker programming or drug regimens were made in 62% of visits in the active vs. 29% in the control group (P < 0.001). Quality of life remained unchanged in both groups.
Conclusion: Remote monitoring was a safe alternative to conventional care and significantly lowered the number of ambulatory visits during long-term follow-up of permanently paced patients. ClinicalTrials.gov identifier: NCT00989326.
Figures
References
-
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA 3rd, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, Hlatky MA, Newby LK, Page RL, Schoenfeld MH, Silka MJ, Stevenson LW, Sweeney MO, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Faxon DP, Halperin JL, Hiratzka LF, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura RA, Ornato JP, Page RL, Riegel B, Tarkington LG, Yancy CW American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices); American Association for Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002. Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;27:e1–e62. 51. - PubMed
-
- Vardas PE, Auricchio A, Blanc JJ European Society of Cardiology; European Heart Rhythm Association. Guidelines for cardiac pacing and cardiac resynchronization therapy. The Task Force for Cardiac Pacing and Cardiac Resynchronization Therapy of the European Society of Cardiology. Developed in collaboration with the European Heart Rhythm Association. Europace. 2007;9:959–998. - PubMed
-
- Heidbüchel H, Lioen P, Foulon S, Huybrechts W, Ector J, Willems R, Ector H. Potential role of remote monitoring for scheduled and unscheduled evaluations of patients with an implantable defibrillator. Europace. 2008;10:351–357. - PubMed
-
- Wallbrück K, Stellbrink C, Santini M, Gill J, Hartmann A, Wunderlich E. The value of permanent follow-up of implantable pacemakers—first results of an European trial. Biomed Tech (Berl) 2002;47:950–953. - PubMed
