

A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus
- PMID: 22127708
- PMCID: PMC5007058
- DOI: 10.1002/art.30613
A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus
Abstract
Objective: To assess the efficacy/safety of the B lymphocyte stimulator inhibitor belimumab plus standard therapy compared with placebo plus standard therapy in active systemic lupus erythematosus (SLE).
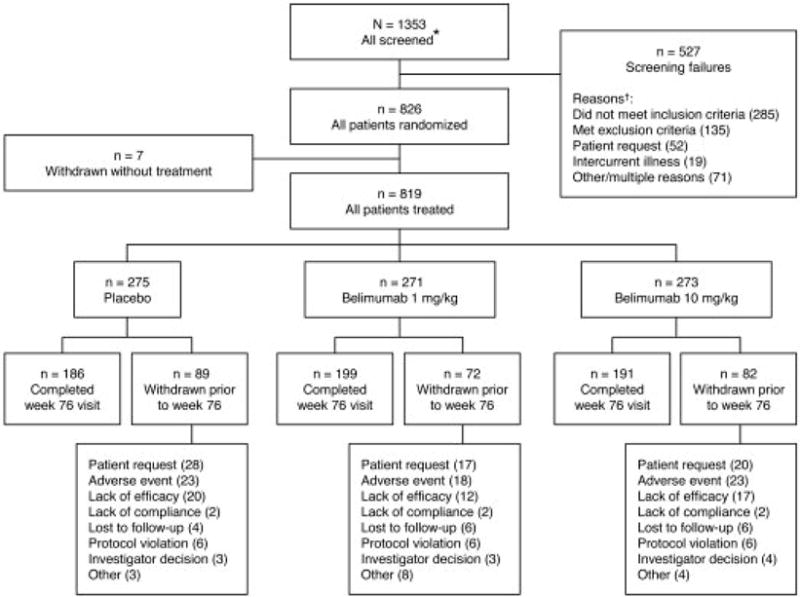
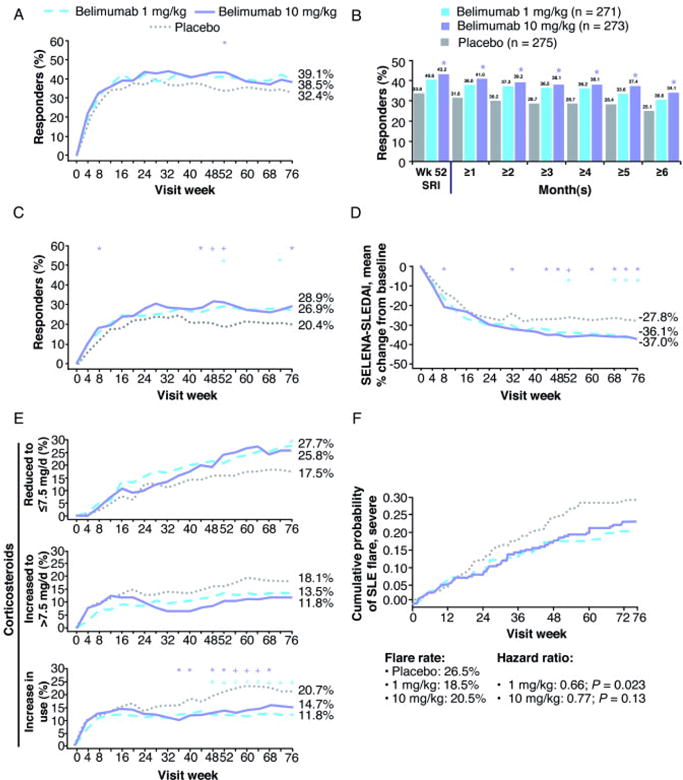
Methods: In a phase III, multicenter, randomized, placebo-controlled trial, 819 antinuclear antibody-positive or anti-double-stranded DNA-positive SLE patients with scores ≥6 on the Safety of Estrogens in Lupus Erythematosus National Assessment (SELENA) version of the SLE Disease Activity Index (SLEDAI) were randomized in a 1:1:1 ratio to receive 1 mg/kg belimumab, 10 mg/kg belimumab, or placebo intravenously on days 0, 14, and 28 and then every 28 days for 72 weeks. The primary efficacy end point was the SLE Responder Index (SRI) response rate at week 52 (an SRI response was defined as a ≥4-point reduction in SELENA-SLEDAI score, no new British Isles Lupus Assessment Group [BILAG] A organ domain score and no more than 1 new BILAG B score, and no worsening in physician's global assessment score versus baseline).
Results: Belimumab at 10 mg/kg plus standard therapy met the primary efficacy end point, generating a significantly greater SRI response at week 52 compared with placebo (43.2% versus 33.5%; P = 0.017). The rate with 1 mg/kg belimumab was 40.6% (P = 0.089). Response rates at week 76 were 32.4%, 39.1%, and 38.5% with placebo, 1 mg/kg belimumab, and 10 mg/kg belimumab, respectively. In post hoc sensitivity analyses evaluating higher SELENA-SLEDAI score thresholds, 10 mg/kg belimumab achieved better discrimination at weeks 52 and 76. Risk of severe flares over 76 weeks (based on the modified SLE Flare Index) was reduced with 1 mg/kg belimumab (34%) (P = 0.023) and 10 mg/kg belimumab (23%) (P = 0.13). Serious and severe adverse events, including infections, laboratory abnormalities, malignancies, and deaths, were comparable across groups.
Conclusion: Belimumab plus standard therapy significantly improved SRI response rate, reduced SLE disease activity and severe flares, and was generally well tolerated in SLE.
Trial registration: ClinicalTrials.gov NCT00410384.
Copyright © 2011 by the American College of Rheumatology.
Conflict of interest statement
The other authors declare that they have no conflicts of interest.
Figures
References
-
- ACR Ad Hoc Committee on Systemic Lupus Erythematosus Guidelines. Guidelines for the referral and management of systemic lupus erythematosus in adults. Arthritis Rheum. 1999;42:1785–96. - PubMed
-
- Bernatsky S, Boivin JF, Joseph L, Manzi S, Ginzler E, Gladman DD, et al. Mortality in systemic lupus erythematosus. Arthritis Rheum. 2006;54:2550–7. - PubMed
-
- D’Cruz DP, Khamashta MA, Hughes GRV. Systemic lupus erythematosus. Lancet. 2007;369:587–96. - PubMed
-
- Lau CS, Mak A. The socioeconomic burden of SLE. Nat Rev Rheumatol. 2009;5:400–4. - PubMed
-
- Browning JL. B cells move to centre stage: novel opportunities for autoimmune disease treatment. Nat Rev Drug Disc. 2006;5:564–76. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
