

CT in the clinical and prognostic evaluation of acute graft-vs-host disease of the gastrointestinal tract
- PMID: 22128129
- PMCID: PMC3587078
- DOI: 10.1259/bjr/60038597
CT in the clinical and prognostic evaluation of acute graft-vs-host disease of the gastrointestinal tract
Abstract
Objective: To determine the role of abdominal CT in assessment of severity and prognosis of patients with acute gastrointestinal (GI) graft-vs-host disease (GVHD).
Methods: During 2000-2004, 41 patients with a clinical diagnosis of acute GI-GVHD were evaluated. CTs were examined for intestinal and extra-intestinal abnormalities, and correlated with clinical staging and outcome.
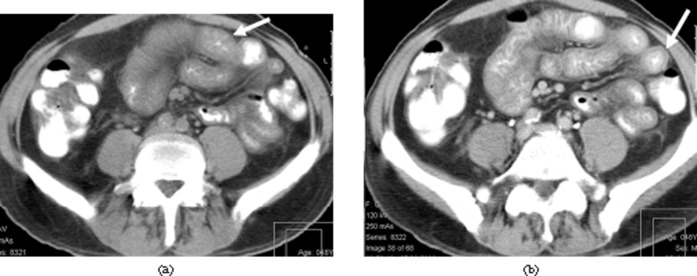
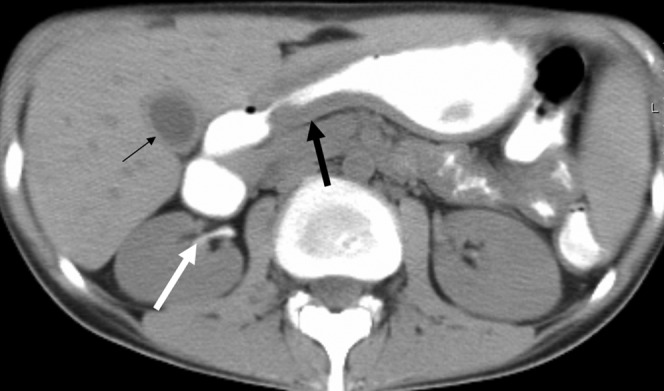
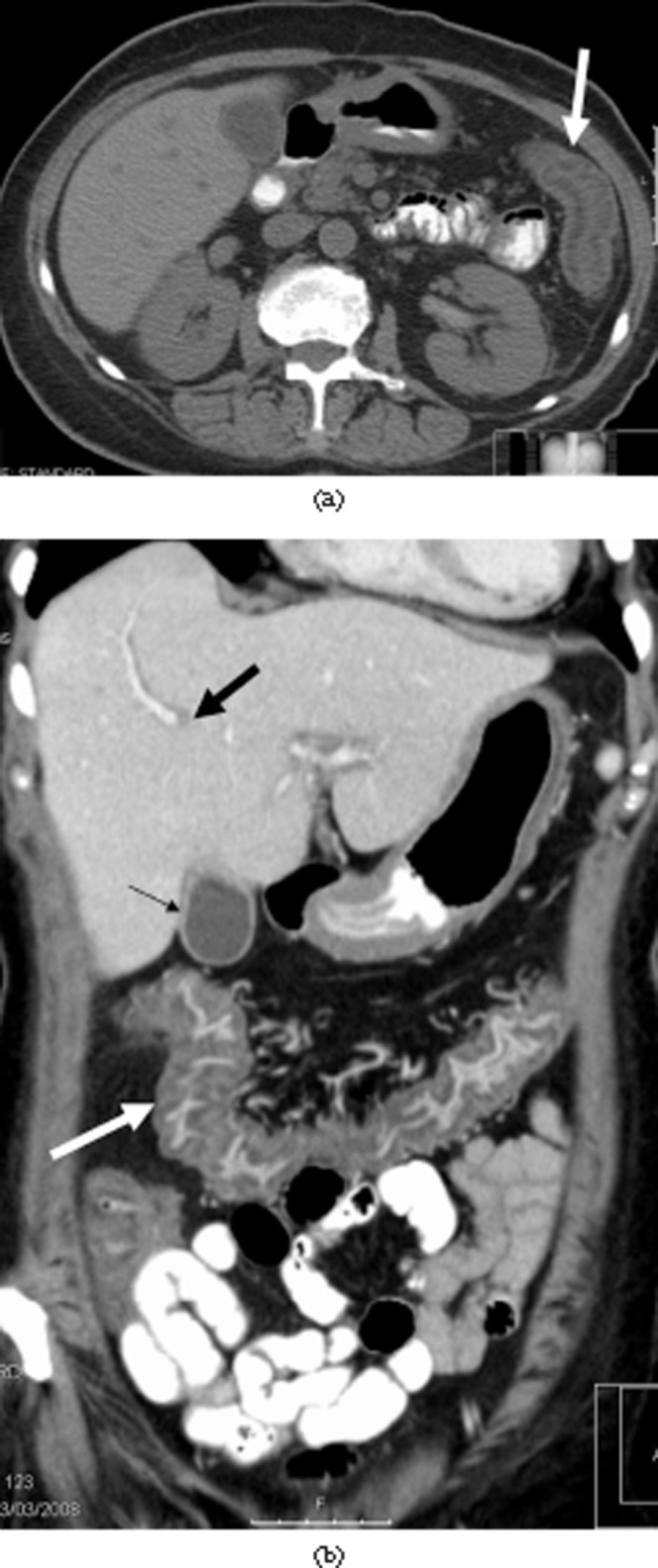
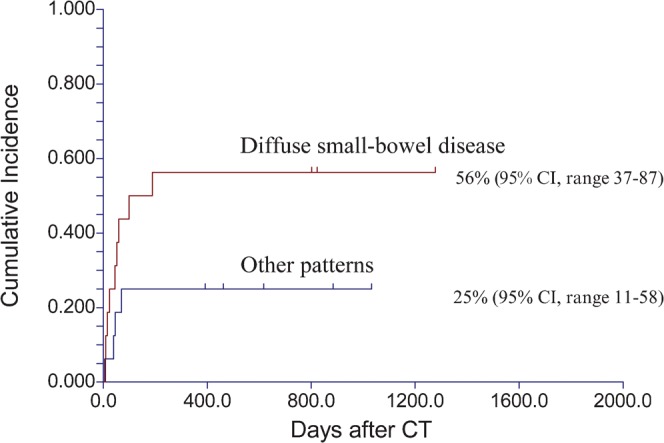
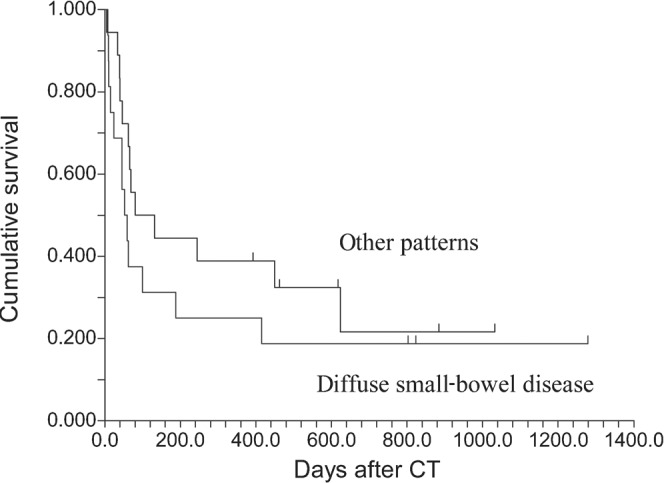
Results: 20 patients had GVHD clinical Stage I-II and 21 had Stage III-IV. 39 (95%) had abnormal CT appearances. The most consistent finding was bowel wall thickening: small (n=14, 34%) or large (n=5, 12%) bowel, or both (n=20, 49%). Other manifestations included bowel dilatation (n=7, 17%), mucosal enhancement (n=6, 15%) and gastric wall thickening (n=9, 38%). Extra-intestinal findings included mesenteric stranding (n=25, 61%), ascites (n=17, 41%), biliary abnormalities (n=12, 29%) and urinary excretion of orally administered gastrografin (n=12, 44%). Diffuse small-bowel thickening and any involvement of the large bowel were associated with severe clinical presentation. Diffuse small-bowel disease correlated with poor prognosis. 8 of 21 patients responded to therapy, compared with 15 of 20 patients with other patterns (p=0.02), and the cumulative incidence of GVHD-related death was 62% and 24%, respectively (p=0.01). Overall survival was not significantly different between patients with diffuse small-bowel disease and patients with other patterns (p=0.31). Colonic disease correlated with severity of GVHD (p=0.04), but not with response to therapy or prognosis (p=0.45).
Conclusion: GVHD often presented with abdominal CT abnormalities. Diffuse small-bowel disease was associated with poor therapeutic response. CT may play a role in supporting clinical diagnosis of GI GVHD and determining prognosis.
Figures


Similar articles
-
Early and late-onset acute GvHD following hematopoietic cell transplantation: CT features of gastrointestinal involvement with clinical and pathological correlation.Eur J Radiol. 2010 Mar;73(3):594-600. doi: 10.1016/j.ejrad.2009.01.011. Epub 2009 Feb 6. Eur J Radiol. 2010. PMID: 19201121
-
CT features with pathologic correlation of acute gastrointestinal graft-versus-host disease after bone marrow transplantation in adults.AJR Am J Roentgenol. 2003 Dec;181(6):1621-5. doi: 10.2214/ajr.181.6.1811621. AJR Am J Roentgenol. 2003. PMID: 14627585
-
Crypt loss is a marker of clinical severity of acute gastrointestinal graft-versus-host disease.Am J Hematol. 2007 Oct;82(10):881-6. doi: 10.1002/ajh.20976. Am J Hematol. 2007. PMID: 17570511
-
CT features of peripheral T-cell lymphoma in the gastrointestinal tract in Chinese population and literature review.J Med Imaging Radiat Oncol. 2012 Apr;56(2):143-50. doi: 10.1111/j.1754-9485.2011.02329.x. J Med Imaging Radiat Oncol. 2012. PMID: 22498185 Review.
-
Prophylaxis and management of graft versus host disease after stem-cell transplantation for haematological malignancies: updated consensus recommendations of the European Society for Blood and Marrow Transplantation.Lancet Haematol. 2020 Feb;7(2):e157-e167. doi: 10.1016/S2352-3026(19)30256-X. Lancet Haematol. 2020. PMID: 32004485 Review.
Cited by
-
PET assessment of acute gastrointestinal graft versus host disease.Bone Marrow Transplant. 2023 Sep;58(9):973-979. doi: 10.1038/s41409-023-02038-9. Epub 2023 Aug 3. Bone Marrow Transplant. 2023. PMID: 37537245 Free PMC article. Review.
-
Intestinal and Extraintestinal Findings of Graft-versus-Host Disease on CT: A Case Series with Radiological and Histopathological Correlations.Biomedicines. 2024 Jul 8;12(7):1516. doi: 10.3390/biomedicines12071516. Biomedicines. 2024. PMID: 39062089 Free PMC article.
-
Advances in Imaging of Inflammation, Fibrosis, and Cancer in the Gastrointestinal Tract.Int J Mol Sci. 2022 Dec 17;23(24):16109. doi: 10.3390/ijms232416109. Int J Mol Sci. 2022. PMID: 36555749 Free PMC article. Review.
-
Gastrointestinal bleeding: imaging and interventions in cancer patients.Br J Radiol. 2022 Jul 1;95(1135):20211158. doi: 10.1259/bjr.20211158. Epub 2022 May 9. Br J Radiol. 2022. PMID: 35451853 Free PMC article. Review.
-
Diagnostic prediction of gastrointestinal graft-versus-host disease based on a clinical- CT- signs nomogram model.Insights Imaging. 2024 Mar 22;15(1):84. doi: 10.1186/s13244-024-01654-3. Insights Imaging. 2024. PMID: 38517664 Free PMC article.
References
-
- Martin PJ, Hansen JA, Strob R, Thomas ED. Human marrow transplantation: an immunological perspective. Adv Immunol 1987;40:379–438 - PubMed
-
- Beatty PG, Dahlberg S, Mickelson EM, Nisperos B, Opelz G, Martin PJ, et al. Probability of finding HLA-matched unrelated marrow donors. Transplantation 1988;45:714–18 - PubMed
-
- Armitage JO. Bone marrow transplantation. N Engl J Med 1994;330:827–38 - PubMed
-
- Thomas ED. Bone marrow transplantation: a review. Semin Hematol 1999;36:95–103 - PubMed
-
- Tabbara IA, Zimmerman K, Morgan C, Nahleh Z. Allogeneic hematopoietic stem cell transplantation. Complications and results. Arch Intern Med 2002;162:1558–66 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
