

Resting energy expenditure and nutritional status in patients undergoing transthoracic esophagectomy for esophageal cancer
- PMID: 22128215
- PMCID: PMC3208012
- DOI: 10.3164/jcbn.11-13
Resting energy expenditure and nutritional status in patients undergoing transthoracic esophagectomy for esophageal cancer
Abstract
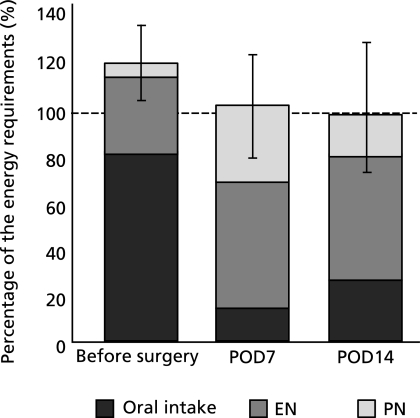
This study was to assess the resting energy expenditure of patients with esophageal cancer using indirect calorimetry. Eight male patients with esophageal cancer and eight male healthy controls were enrolled in this study. All patients underwent transthoracic esophagectomy with lymph nodes dissections. The resting energy expenditure was measured preoperatively, and on postoperative day 7 and 14 using indirect calorimetry. Preoperatively, the measured resting energy expenditure/body weight in these patients was significantly higher than that of the controls (23.3 ± 2.1 kcal/kg/day vs 20.4 ± 1.6 kcal/kg/day), whereas the measured/predicted energy expenditure from the Harris-Benedict equation ratio was 1.01 ± 0.09, which did not differ significantly from the control values. The measured resting energy expenditure/body weight was 27.3 ± 3.5 kcal/kg/day on postoperative day 7, and 23.7 ± 5.07 kcal/kg/day on postoperative day 14. Significant increases in the measured resting energy expenditure were observed on postoperative day 7, and the measured/predicted energy expenditure ratio was 1.17 ± 0.15. In conclusion, patients with operable esophageal cancers were almost normometabolic before surgery. On the other hand, the patients showed a hyper-metabolic status after esophagectomy. We recommended that nutritional management based on 33 kcal/body weight/day (calculated by the measured resting energy expenditure × active factor 1.2-1.3) may be optimal for patients undergoing esophagectomy.
Keywords: esophagectomy; indirect calorimetry; resting energy expenditure.
Figures




Similar articles
-
Resting energy expenditure in patients undergoing pylorus preserving pancreatoduodenectomies for bile duct cancer or pancreatic tumors.J Clin Biochem Nutr. 2011 May;48(3):183-6. doi: 10.3164/jcbn.10-83. Epub 2011 Apr 13. J Clin Biochem Nutr. 2011. PMID: 21562636 Free PMC article.
-
Energy expenditure in Japanese patients with severe or moderate ulcerative colitis.J Clin Biochem Nutr. 2010 Jul;47(1):32-6. doi: 10.3164/jcbn.10-07. Epub 2010 Apr 23. J Clin Biochem Nutr. 2010. PMID: 20664728 Free PMC article.
-
Validation of a predictive method for an accurate assessment of resting energy expenditure in medical mechanically ventilated patients.Crit Care Med. 2008 Apr;36(4):1175-83. doi: 10.1097/CCM.0b013e3181691502. Crit Care Med. 2008. PMID: 18379244 Clinical Trial.
-
Energy metabolism in Japanese patients with Crohn's disease.J Clin Biochem Nutr. 2010 Jan;46(1):68-72. doi: 10.3164/jcbn.09-55. Epub 2009 Dec 29. J Clin Biochem Nutr. 2010. PMID: 20104267 Free PMC article.
-
The agreement between measured and predicted resting energy expenditure in patients with pancreatic cancer: a pilot study.JOP. 2004 Jan;5(1):32-40. JOP. 2004. PMID: 14730120
Cited by
-
Changes in energy metabolism after induction therapy in patients with severe or moderate ulcerative colitis.J Clin Biochem Nutr. 2015 May;56(3):215-9. doi: 10.3164/jcbn.14-100. Epub 2015 Mar 28. J Clin Biochem Nutr. 2015. PMID: 26060352 Free PMC article.
-
Sarcopenia is a predictive factor for intestinal resection in admitted patients with Crohn's disease.PLoS One. 2017 Jun 23;12(6):e0180036. doi: 10.1371/journal.pone.0180036. eCollection 2017. PLoS One. 2017. PMID: 28644887 Free PMC article.
-
Energy metabolism and nutritional status in hospitalized patients with lung cancer.J Clin Biochem Nutr. 2016 Sep;59(2):122-129. doi: 10.3164/jcbn.16-1. Epub 2016 Jul 26. J Clin Biochem Nutr. 2016. PMID: 27698539 Free PMC article.
-
Assessment of the Physical Invasiveness of Peroral Endoscopic Myotomy during the Perioperative Period Based on Changes in Energy Metabolism.Metabolites. 2023 Aug 23;13(9):969. doi: 10.3390/metabo13090969. Metabolites. 2023. PMID: 37755250 Free PMC article.
-
Estimation of perioperative invasiveness of colorectal endoscopic submucosal dissection evaluated by energy metabolism.J Clin Biochem Nutr. 2018 Sep;63(2):164-167. doi: 10.3164/jcbn.18-12. Epub 2018 Apr 11. J Clin Biochem Nutr. 2018. PMID: 30279629 Free PMC article.
References
-
- Bozzetti F, von Meyenfeldt MF. Nutritional support in cancer. In: Lubos Sobotka., editor. Basic in Clinical Nutrition Third Edition. Prague: Publishing House Galen; 2004. pp. 392–402.
-
- Tisdale MJ. Cachexia in cancer patients. Nat Rev Cancer. 2002;2:862–871. - PubMed
-
- Dempsey DT, Feurer ID, Knox LS, Crosby LO, Buzby GP, Mullen JL. Energy expenditure in malnourished gastrointestinal cancer patients. Cancer. 1984;53:1265–1273. - PubMed