

Mother-to-child transmission of human immunodeficiency virus in aten years period
- PMID: 22129112
- PMCID: PMC3247874
- DOI: 10.1186/1742-4755-8-35
Mother-to-child transmission of human immunodeficiency virus in aten years period
Abstract
Objectives: to evaluate mother-to-child transmission (MTCT) rates and related factors in HIV-infected pregnant women from a tertiary hospital between 2000 and 2009.
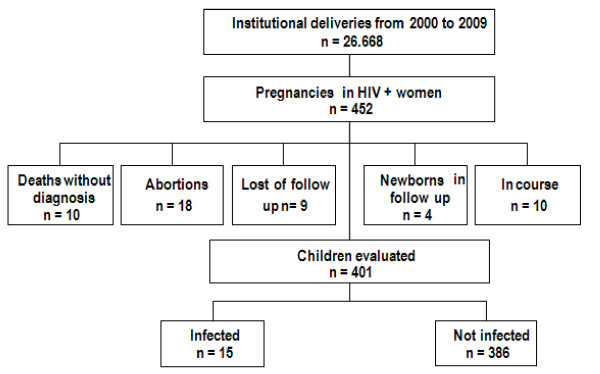
Subjects and method: cohort of 452 HIV-infected pregnant women and their newborns. Data was collected from recorded files and undiagnosed children were enrolled for investigation.
Statistical analysis: qui-square test, Fisher exact test, Student t test, Mann-Whitney test, ANOVA, risk ratio and confidence intervals.
Results: MTCT occurred in 3.74%. The study population displayed a mean age of 27 years; 86.5% were found to have acquired HIV through sexual contact; 55% were aware of the diagnosis prior to the pregnancy; 62% were not using HAART. Mean CD4 cell-count was 474 cells/ml and 70.3% had undetectable viral loads in the third trimester. HAART included nevirapine in 35% of cases and protease inhibitors in 55%; Zidovudine monotherapy was used in 7.3%. Mean gestational age at delivery was 37.2 weeks and in 92% by caesarian section; 97.2% received intravenous zidovudine. Use of AZT to newborn occurred in 100% of them. Factors identified as associated to MTCT were: low CD4 cell counts, elevated viral loads, maternal AIDS, shorter periods receiving HAART, other conditions (anemia, IUGR (intra uterine growth restriction), oligohydramnium), coinfecctions (CMV and toxoplasmosis) and the occurrence of labor. Use of HAART for longer periods, caesarian and oral zidovudine for the newborns were associated with a decreased risk. Poor adhesion to treatment was present in 13 of the 15 cases of transmission; in 7, coinfecctions were diagnosed (CMV and toxoplasmosis).
Conclusion: Use of HAART and caesarian delivery are protective factors for mother-to-child transmission of HIV. Maternal coinfecctions and other conditions were risk factors for MTCT.
Figures
References
-
- WHO. Joint United Nations Programme on HIV/AIDS (UNAIDS) Report on the Global AIDS Epidemic: 2010. Geneva. 2010.
-
- Szwarcwald CL, Júnior AB, Souza-Júnior PRB, Lemos KRV, Frias PG, Luhm KR. et al.HIV Testing During Pregnancy: Use of Secondary Data to Estimate 2006 Test Coverage and Prevalence in Brazil. The Braz J Infect Dis. 2008;12(3):167–172. - PubMed
-
- Succi RCM. Mother-to-child transmission of HIV in Brazil during the years 2000 and 2001: results of a multi-centric study. Cad Saúde Pública. 2007;23(3):379–389. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
