

Are radiologists' goals for mammography accuracy consistent with published recommendations?
- PMID: 22130089
- PMCID: PMC3274618
- DOI: 10.1016/j.acra.2011.10.013
Are radiologists' goals for mammography accuracy consistent with published recommendations?
Abstract
Rationale and objectives: Mammography quality assurance programs have been in place for more than a decade. We studied radiologists' self-reported performance goals for accuracy in screening mammography and compared them to published recommendations.
Materials and methods: A mailed survey of radiologists at mammography registries in seven states within the Breast Cancer Surveillance Consortium (BCSC) assessed radiologists' performance goals for interpreting screening mammograms. Self-reported goals were compared to published American College of Radiology (ACR) recommended desirable ranges for recall rate, false-positive rate, positive predictive value of biopsy recommendation (PPV2), and cancer detection rate. Radiologists' goals for interpretive accuracy within desirable range were evaluated for associations with their demographic characteristics, clinical experience, and receipt of audit reports.
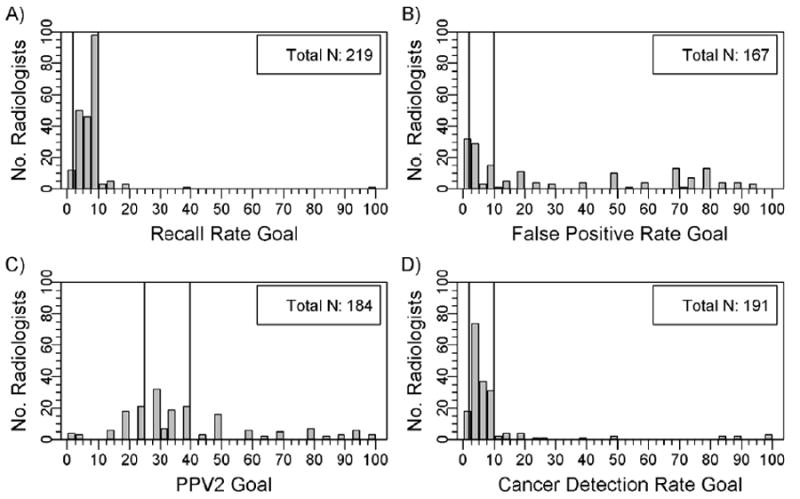
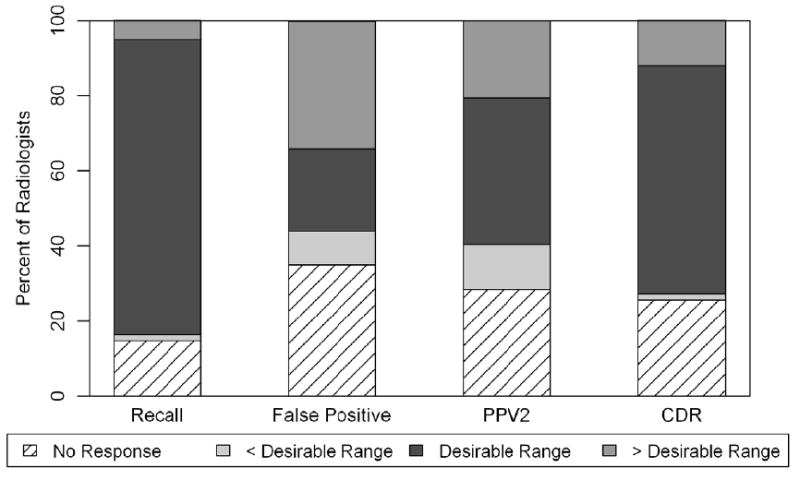
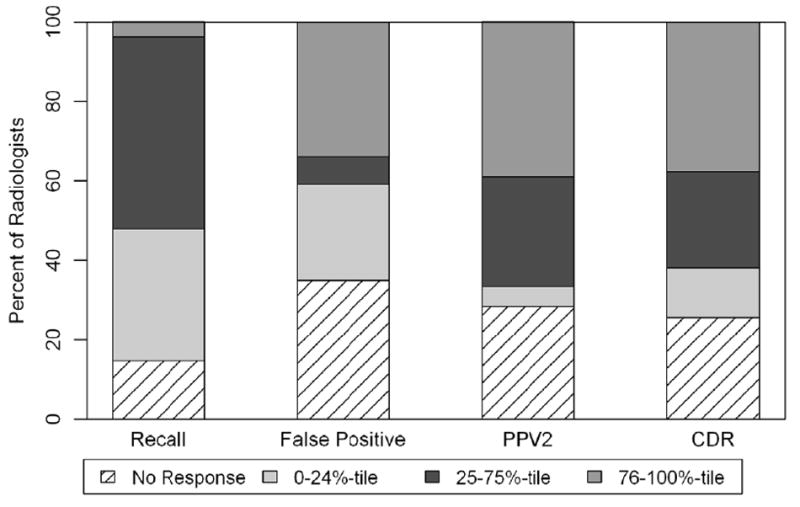
Results: The survey response rate was 71% (257 of 364 radiologists). The percentage of radiologists reporting goals within desirable ranges was 79% for recall rate, 22% for false-positive rate, 39% for PPV2, and 61% for cancer detection rate. The range of reported goals was 0%-100% for false-positive rate and PPV2. Primary academic affiliation, receiving more hours of breast imaging continuing medical education, and receiving audit reports at least annually were associated with desirable PPV2 goals. Radiologists reporting desirable cancer detection rate goals were more likely to have interpreted mammograms for 10 or more years, and >1000 mammograms per year.
Conclusion: Many radiologists report goals for their accuracy when interpreting screening mammograms that fall outside of published desirable benchmarks, particularly for false-positive rate and PPV2, indicating an opportunity for education.
Copyright © 2012 AUR. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Radiologists' attitudes and use of mammography audit reports.Acad Radiol. 2010 Jun;17(6):752-60. doi: 10.1016/j.acra.2010.02.010. Acad Radiol. 2010. PMID: 20457418 Free PMC article.
-
Variability in interpretive performance at screening mammography and radiologists' characteristics associated with accuracy.Radiology. 2009 Dec;253(3):641-51. doi: 10.1148/radiol.2533082308. Epub 2009 Oct 28. Radiology. 2009. PMID: 19864507 Free PMC article.
-
Effect of radiologists' diagnostic work-up volume on interpretive performance.Radiology. 2014 Nov;273(2):351-64. doi: 10.1148/radiol.14132806. Epub 2014 Jun 24. Radiology. 2014. PMID: 24960110 Free PMC article.
-
Radiologists' interpretive efficiency and variability in true- and false-positive detection when screen-reading with tomosynthesis (3D-mammography) relative to standard mammography in population screening.Breast. 2015 Dec;24(6):687-93. doi: 10.1016/j.breast.2015.08.012. Epub 2015 Oct 1. Breast. 2015. PMID: 26433751 Review.
-
Statistical approaches for modeling radiologists' interpretive performance.Acad Radiol. 2009 Feb;16(2):227-38. doi: 10.1016/j.acra.2008.07.022. Acad Radiol. 2009. PMID: 19124109 Free PMC article. Review.
Cited by
-
Comparing search patterns in digital breast tomosynthesis and full-field digital mammography: an eye tracking study.J Med Imaging (Bellingham). 2017 Oct;4(4):045501. doi: 10.1117/1.JMI.4.4.045501. Epub 2017 Oct 27. J Med Imaging (Bellingham). 2017. PMID: 29098168 Free PMC article.
-
How one block of trials influences the next: persistent effects of disease prevalence and feedback on decisions about images of skin lesions in a large online study.Cogn Res Princ Implic. 2022 Feb 2;7(1):10. doi: 10.1186/s41235-022-00362-0. Cogn Res Princ Implic. 2022. PMID: 35107667 Free PMC article.
-
Effects of blinded and nonblinded sequential human redundancy on inspection effort and inspection outcome in low prevalence visual search.Sci Rep. 2024 Oct 3;14(1):23003. doi: 10.1038/s41598-024-72210-8. Sci Rep. 2024. PMID: 39362903 Free PMC article.
-
Breast cancer mammographic diagnosis performance in a public health institution: a retrospective cohort study.Insights Imaging. 2017 Dec;8(6):581-588. doi: 10.1007/s13244-017-0573-2. Epub 2017 Oct 4. Insights Imaging. 2017. PMID: 28980214 Free PMC article.
-
Mammographic interpretation: radiologists' ability to accurately estimate their performance and compare it with that of their peers.AJR Am J Roentgenol. 2012 Sep;199(3):695-702. doi: 10.2214/AJR.11.7402. AJR Am J Roentgenol. 2012. PMID: 22915414 Free PMC article.
References
-
- Feig SA. Auditing and benchmarks in screening and diagnostic mammography. Radiol Clin North Am. 2007;45(5):791–800. vi. - PubMed
-
- American College of Radiology. ACR BI-RADS - Mammography. 4. Reston, VA: American College of Radiology; 2003.
-
- Perry N, Broeders M, de Wolf C, Tornberg S, Holland R, von Karsa L. European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition--summary document. Ann Oncol. 2008;19(4):614–622. - PubMed
-
- US Food and Drug Administration/Center for Devices and Radiological Health. [2 May, 2011];US FDA/CDRH: Mammography Program. Available at: http://www.fda.gov/cdrh/mammography.
-
- EUREF European Reference Organisation for Quality Assured Breast Screening and Diagnostic Services. [Accessed 2 May, 2011]; Available at: http://www.euref.org/
Publication types
MeSH terms
Grants and funding
- U01 CA063740/CA/NCI NIH HHS/United States
- U01CA69976/CA/NCI NIH HHS/United States
- U01 CA070040/CA/NCI NIH HHS/United States
- R01 AA010762/AA/NIAAA NIH HHS/United States
- U01CA63736/CA/NCI NIH HHS/United States
- U01CA86082/CA/NCI NIH HHS/United States
- K05 CA104699/CA/NCI NIH HHS/United States
- R01 AT010762/AT/NCCIH NIH HHS/United States
- U01CA70040/CA/NCI NIH HHS/United States
- U01CA63740/CA/NCI NIH HHS/United States
- U01CA70013/CA/NCI NIH HHS/United States
- R01 CA140560/CA/NCI NIH HHS/United States
- R01 CA107623/CA/NCI NIH HHS/United States
- 1R01 CA10762/CA/NCI NIH HHS/United States
- U01 CA086082/CA/NCI NIH HHS/United States
- U01 CA063731/CA/NCI NIH HHS/United States
- U01 CA086076/CA/NCI NIH HHS/United States
- U01 CA069976/CA/NCI NIH HHS/United States
- U01CA86076/CA/NCI NIH HHS/United States
- U01 CA063736/CA/NCI NIH HHS/United States
- 1K05 CA104699/CA/NCI NIH HHS/United States
- U01 CA070013/CA/NCI NIH HHS/United States
- U01CA63731/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
