Superimposed fungal ulcer after fibrin glue sealant in infectious corneal ulcer
- PMID: 22131784
- PMCID: PMC3223714
- DOI: 10.3341/kjo.2011.25.6.447
Superimposed fungal ulcer after fibrin glue sealant in infectious corneal ulcer
Abstract
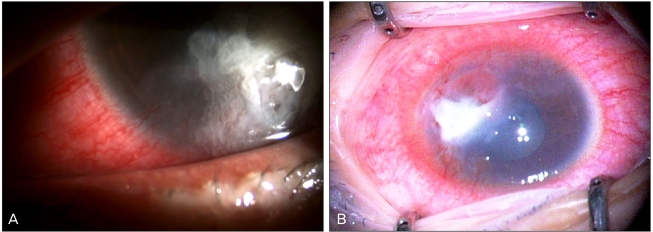
A healthy 27-year-old woman with a corneal ulcer underwent fibrin gluing with a bandage contact lens twice, due to an impending perforation. The ulcer lesion slowly progressed, unresponsive to topical antibiotics and amphotericin B. We removed the gluing patch and performed a corneal or scraping or biopsy with multiple amniotic membrane grafts to seal the thinned or perforated cornea. Three days after the surgery, the corneal cultures grew Fusarium, as well as Enterococcus faecalis. Three weeks after surgery, the outermost layer of amniotic membranes, serving as a temporary patch, was removed. The anterior chamber was clear without cells. The signs of infection clinically and symptomatically cleared up four weeks later. Two months after surgery, the lesion became enhanced by amniotic membranes. The use of fibrin glue in infectious keratitis should be avoided, because it not only masks the underlying lesion, but it also interferes with drug penetration into the underlying lesion.
Keywords: Corneal perforation; Corneal ulcer; Fibrin glue; Tissue adhesives; Tissue glue.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

Similar articles
-
Adjunctive Oral Voriconazole Treatment of Fusarium Keratitis: A Secondary Analysis From the Mycotic Ulcer Treatment Trial II.JAMA Ophthalmol. 2017 Jun 1;135(6):520-525. doi: 10.1001/jamaophthalmol.2017.0616. JAMA Ophthalmol. 2017. PMID: 28426856 Free PMC article. Clinical Trial.
-
Antimicrobial efficacy of corneal cross-linking in vitro and in vivo for Fusarium solani: a potential new treatment for fungal keratitis.BMC Ophthalmol. 2018 Mar 2;18(1):65. doi: 10.1186/s12886-018-0727-0. BMC Ophthalmol. 2018. PMID: 29499665 Free PMC article.
-
Conjunctival Hyperemia or Vasodilation and Central Corneal Ulcer in a Neonate.JAMA Ophthalmol. 2018 May 1;136(5):589-590. doi: 10.1001/jamaophthalmol.2017.5159. JAMA Ophthalmol. 2018. PMID: 29494721 Free PMC article. No abstract available.
-
A fibrin-related line of research and theoretical possibilities for the use of fibrin glue as a temporary basal membrane in non-perforated corneal ulcers and in photorefractive keratectomy (PRK)-operated corneas.Arq Bras Oftalmol. 2007 Sep-Oct;70(5):884-9. doi: 10.1590/s0004-27492007000500029. Arq Bras Oftalmol. 2007. PMID: 18157320 Review.
-
[Use of a fibrin glue (Tissucol) for treating perforated or pre-perforated corneal ulcer].J Fr Ophtalmol. 1989;12(6-7):469-76. J Fr Ophtalmol. 1989. PMID: 2699886 Review. French.
Cited by
-
Repeated Freezing Procedures Preserve Structural and Functional Properties of Amniotic Membrane for Application in Ophthalmology.Int J Mol Sci. 2020 Jun 4;21(11):4029. doi: 10.3390/ijms21114029. Int J Mol Sci. 2020. PMID: 32512889 Free PMC article.
-
Sutureless fixation of amniotic membrane for therapy of ocular surface disorders.PLoS One. 2015 May 8;10(5):e0125035. doi: 10.1371/journal.pone.0125035. eCollection 2015. PLoS One. 2015. PMID: 25955359 Free PMC article. Clinical Trial.
-
Tissue Adhesives for the Management of Corneal Perforations and Challenging Corneal Conditions.Clin Ophthalmol. 2023 Jan 15;17:209-223. doi: 10.2147/OPTH.S394454. eCollection 2023. Clin Ophthalmol. 2023. PMID: 36685088 Free PMC article. Review.
References
-
- Refojo MF, Dohlman CH, Ahmad B, et al. Evaluation of adhesives for corneal surgery. Arch Ophthalmol. 1968;80:645–656. - PubMed
-
- Webster RG, Jr, Slansky HH, Refojo MF, et al. The use of adhesive for the closure of corneal perforations. Report of two cases. Arch Ophthalmol. 1968;80:705–709. - PubMed
-
- Duchesne B, Tahi H, Galand A. Use of human fibrin glue and amniotic membrane transplant in corneal perforation. Cornea. 2001;20:230–232. - PubMed
-
- Sumich PM, Cook SD, Tole DM. Fibrin tissue-filler glue for persistent epithelial defects. Clin Experiment Ophthalmol. 2003;31:267–269. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources