

Bone discrepancy as a powerful indicator for early surgery in obstetric brachial plexus palsy
- PMID: 22131921
- PMCID: PMC2988126
- DOI: 10.1007/s11552-010-9270-z
Bone discrepancy as a powerful indicator for early surgery in obstetric brachial plexus palsy
Abstract
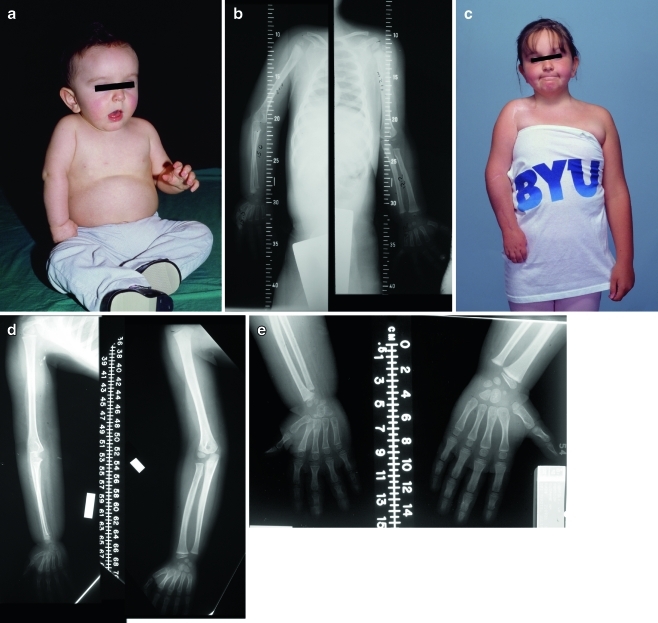
Objectives: One of the unfortunate sequelae in obstetric brachial plexus palsy (OBPP) is upper limb length discrepancy. However, the influence of primary nerve reconstruction remains undetermined. In this study, the resultant discrepancy in children with OBPP who underwent primary reconstruction was analyzed in relation to the severity of the lesion, the timing of surgery, and the functional outcome following surgery.
Methods: Fifty-four patients that met the inclusion criteria were included in this study. Preoperative and postoperative bilateral scanograms were obtained to document the effect of reinnervation on bone growth. The length of the humerus, ulna, third metacarpal, third proximal phalange, and total limb length were measured and the percentage between the affected and normal side were accessed. Correlations between all the measures of limb length and measures of active motion (i.e., three different classification systems) were performed.
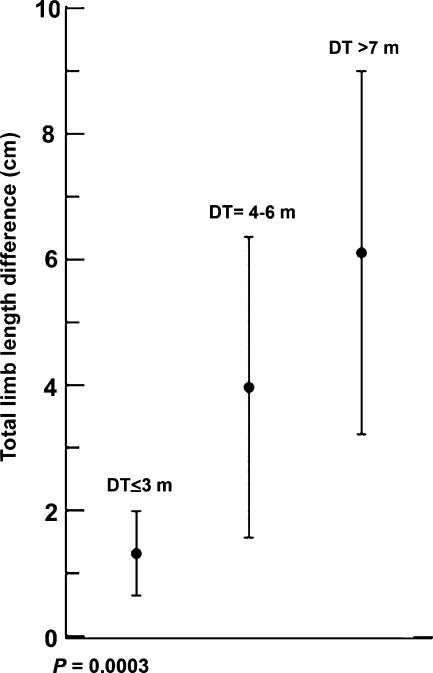
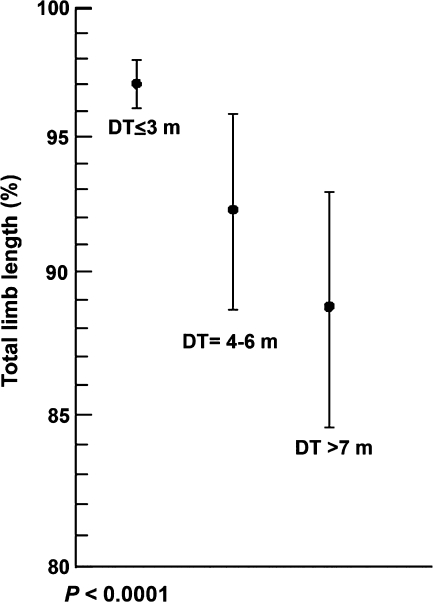
Results: Spearman's rank correlation coefficients revealed significant correlations between limb length discrepancies and nearly all measures of active upper extremity movement. The timing of surgery and the severity of the lesion significantly influenced the resultant limb length discrepancy.
Conclusions: The prevention of a non-acceptable upper limb discrepancy is fundamental for both the patient and family. The extent of the resultant discrepancy appeared to be strongly related to the time between injury and surgery, degree of severity, and the outcome of surgery. Patients with better functional recoveries of the affected upper extremities showed smaller differences in limb length.
Keywords: Functional outcome; Limb length discrepancy; Obstetric brachial plexus palsy; Primary reconstruction.
Figures
References
-
- Boome RS, Kaye JC. Obstetric traction injuries of the brachial plexus. Natural history, indications for surgical repair and results. J Bone Joint Surg Br. 1988;70(4):571–576. - PubMed
-
- Dahl TM. Upper-extremity lengthening. In: Gupta A, Kay SPJ, Scheker LR, editors. The growing hand: diagnosis and management of the upper extremity in children. London: Mosby; 2000. pp. 1049–1056.
-
- Demir SO, Oktay F, Uysal H, Seluk B. Upper extremity shortness in children with hemiplegic cerebral palsy. J Pediatr Orthop. 2006;26(6):764–768. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
