

Accuracy of urine circulating cathodic antigen (CCA) test for Schistosoma mansoni diagnosis in different settings of Côte d'Ivoire
- PMID: 22132246
- PMCID: PMC3222626
- DOI: 10.1371/journal.pntd.0001384
Accuracy of urine circulating cathodic antigen (CCA) test for Schistosoma mansoni diagnosis in different settings of Côte d'Ivoire
Abstract
Background: Promising results have been reported for a urine circulating cathodic antigen (CCA) test for the diagnosis of Schistosoma mansoni. We assessed the accuracy of a commercially available CCA cassette test (designated CCA-A) and an experimental formulation (CCA-B) for S. mansoni diagnosis.
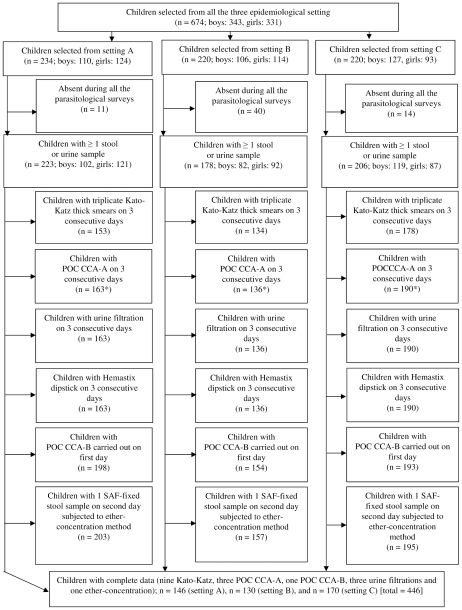
Methodology: We conducted a cross-sectional survey in three settings of Côte d'Ivoire: settings A and B are endemic for S. mansoni, whereas S. haematobium co-exists in setting C. Overall, 446 children, aged 8-12 years, submitted multiple stool and urine samples. For S. mansoni diagnosis, stool samples were examined with triplicate Kato-Katz, whereas urine samples were tested with CCA-A. The first stool and urine samples were additionally subjected to an ether-concentration technique and CCA-B, respectively. Urine samples were examined for S. haematobium using a filtration method, and for microhematuria using Hemastix dipsticks.
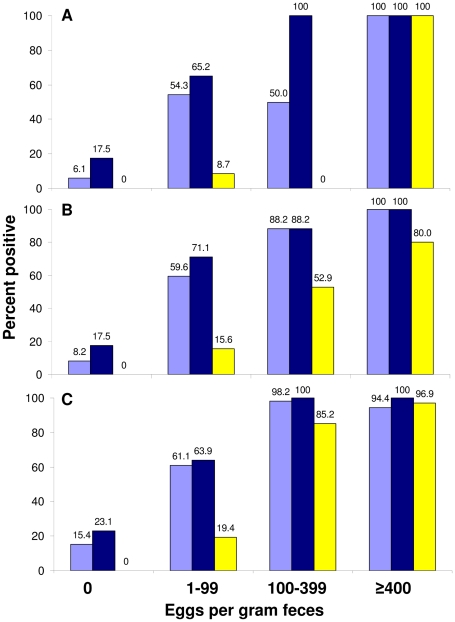
Principal findings: Considering nine Kato-Katz as diagnostic 'gold' standard, the prevalence of S. mansoni in setting A, B and C was 32.9%, 53.1% and 91.8%, respectively. The sensitivity of triplicate Kato-Katz from the first stool and a single CCA-A test was 47.9% and 56.3% (setting A), 73.9% and 69.6% (setting B), and 94.2% and 89.6% (setting C). The respective sensitivity of a single CCA-B was 10.4%, 29.9% and 75.0%. The ether-concentration technique showed a low sensitivity for S. mansoni diagnosis (8.3-41.0%). The specificity of CCA-A was moderate (76.9-84.2%); CCA-B was high (96.7-100%). The likelihood of a CCA-A color reaction increased with higher S. mansoni fecal egg counts (odds ratio: 1.07, p<0.001). A concurrent S. haematobium infection or the presence of microhematuria did not influence the CCA-A test results for S. mansoni diagnosis.
Conclusion/significance: CCA-A showed similar sensitivity than triplicate Kato-Katz for S. mansoni diagnosis with no cross-reactivity to S. haematobium and microhematuria. The low sensitivity of CCA-B in our study area precludes its use for S. mansoni diagnosis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hotez PJ, Molyneux DH, Fenwick A, Kumaresan J, Ehrlich Sachs S, et al. Control of neglected tropical diseases. N Engl J Med. 2007;357:1018–1027. - PubMed
-
- WHO. Preventive chemotherapy in human helminthiasis: coordinated use of anthelminthic drugs in control interventions: a manual for health professionals and programme managers. 2006. World Health Organization, Geneva.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
