

Chest wall reconstruction with strattice in an immunosuppressed patient
- PMID: 22132251
- PMCID: PMC3223486
Chest wall reconstruction with strattice in an immunosuppressed patient
Abstract
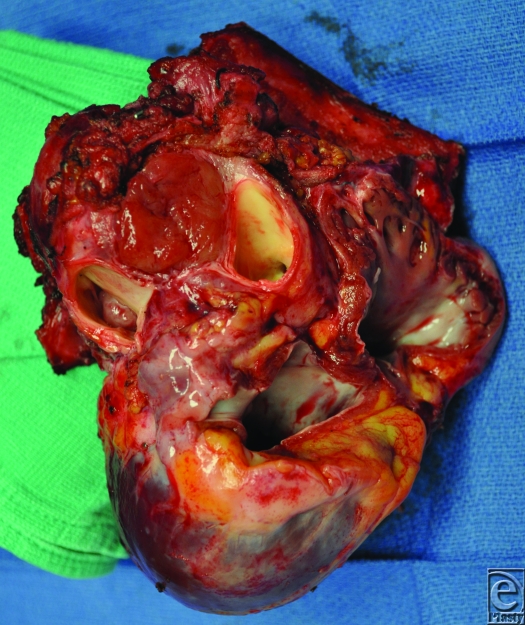
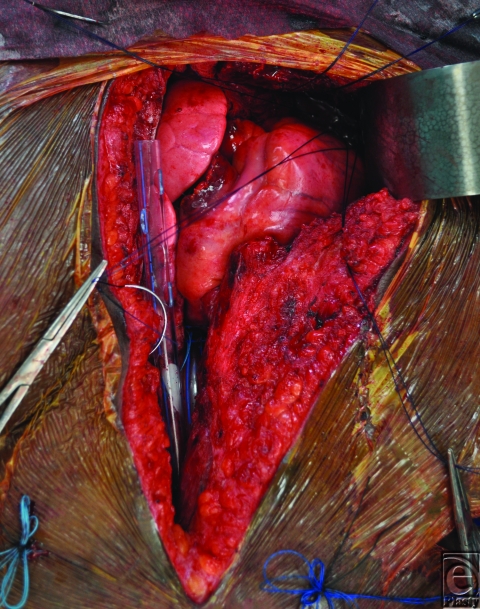
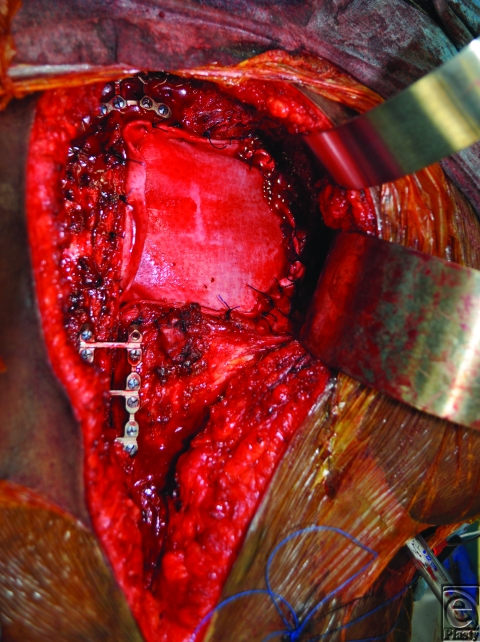
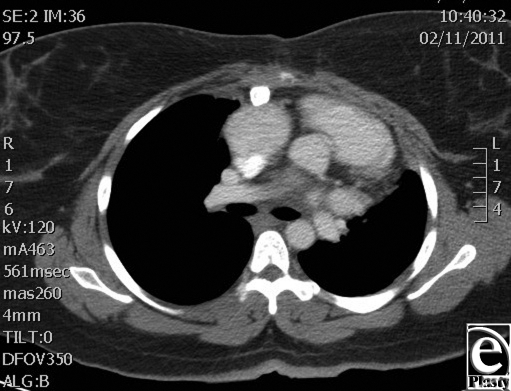
We report successful reconstruction of a challenging composite chest wall defect in an immunocompromised patient using a biologic mesh. Infection results in significant morbidity and mortality in immunocompromised patients. Thus, reconstruction in this population requires careful selection of appropriate materials to repair the defect. A 26-year-old woman with a cardiac paraganglioma required resection of the heart, portions of the great vessels, several ribs, and a large portion of the sternum, with subsequent orthotopic cardiac transplantation. Titanium plates were used to restore sternal continuity and Strattice was used for chest wall reconstruction. Strattice was selected due to its ability to become incorporated and resist wound infection, to provide stability to the rib cage, and to protect the newly transplanted heart. In our experience, Strattice provides a viable alternative to other biologics and is a safer alternative to synthetic mesh for chest wall reconstruction in immunocompromised patients.
Figures

Similar articles
-
Chest Wall Reconstruction with Porcine Acellular Dermal Matrix (Strattice) and Autologous Tissue Transfer for High Risk Patients with Chest Wall Tumors.Plast Reconstr Surg Glob Open. 2018 May 18;6(5):e1703. doi: 10.1097/GOX.0000000000001703. eCollection 2018 May. Plast Reconstr Surg Glob Open. 2018. PMID: 29922541 Free PMC article.
-
Materials and techniques in chest wall reconstruction: a review.J Vis Surg. 2017 Jul 26;3:95. doi: 10.21037/jovs.2017.06.10. eCollection 2017. J Vis Surg. 2017. PMID: 29078657 Free PMC article. Review.
-
Ten-Year Experience of Chest Wall Reconstruction: Retrospective Review of a Titanium Plate MatrixRIB™ System.Front Surg. 2022 Jul 5;9:947193. doi: 10.3389/fsurg.2022.947193. eCollection 2022. Front Surg. 2022. PMID: 35865033 Free PMC article.
-
Three-dimensional printed pure-titanium implantation for chest wall reconstruction involving the sternum and ribs: a novel approach.Interdiscip Cardiovasc Thorac Surg. 2024 Mar 29;38(4):ivae037. doi: 10.1093/icvts/ivae037. Interdiscip Cardiovasc Thorac Surg. 2024. PMID: 38561175 Free PMC article.
-
[Transplantation of allogeneic bone graft in the therapy of massive post-sternotomy defects - 6 years of experience with the method].Rozhl Chir. 2016 Fall;95(11):399-406. Rozhl Chir. 2016. PMID: 28033018 Czech.
Cited by
-
Acellular Dermal Matrices: Applications in Plastic Surgery.Semin Plast Surg. 2019 Aug;33(3):173-184. doi: 10.1055/s-0039-1693019. Epub 2019 Aug 2. Semin Plast Surg. 2019. PMID: 31384233 Free PMC article. Review.
-
Process-induced extracellular matrix alterations affect the mechanisms of soft tissue repair and regeneration.J Tissue Eng. 2013 Sep 10;4:2041731413505305. doi: 10.1177/2041731413505305. eCollection 2013. J Tissue Eng. 2013. PMID: 24555005 Free PMC article.
-
Braxon®-assisted prepectoral breast reconstruction: A decade later.Front Surg. 2022 Nov 1;9:1009356. doi: 10.3389/fsurg.2022.1009356. eCollection 2022. Front Surg. 2022. PMID: 36420412 Free PMC article. Review.
-
Multidisciplinary Oncoplastic Approach Reduces Infection in Chest Wall Resection and Reconstruction for Malignant Chest Wall Tumors.Plast Reconstr Surg Glob Open. 2016 Jul 20;4(7):e809. doi: 10.1097/GOX.0000000000000751. eCollection 2016 Jul. Plast Reconstr Surg Glob Open. 2016. PMID: 27536488 Free PMC article.
-
Chest Wall Reconstruction with Porcine Acellular Dermal Matrix (Strattice) and Autologous Tissue Transfer for High Risk Patients with Chest Wall Tumors.Plast Reconstr Surg Glob Open. 2018 May 18;6(5):e1703. doi: 10.1097/GOX.0000000000001703. eCollection 2018 May. Plast Reconstr Surg Glob Open. 2018. PMID: 29922541 Free PMC article.
References
-
- Hertz MI, Aurora P, Christie JD, et al. Scientific registry of the International Society for Heart and Lung Transplantation: introduction to the 2009 annual reports. J Heart Lung Transplant. 2009;28:989–1049. - PubMed
-
- Arnold PG, Pairolero PC. Chest-wall reconstruction: an account of 500 consecutive patients. Plast Reconstr Surg. 1996;98(5):804–10. - PubMed
-
- Hirai S, Nobuto H, Yokota K, et al. Surgical resection and reconstruction for primary malignant sternal tumor. Ann Thorac Cardiovasc Surg. 2009;15(3):182–5. - PubMed
-
- Chase CW, Franklin JD, Guest DP, Barker DE. Internal fixation of the sternum in median sternotomy dehiscence. Plast Reconstr Surg. 1999;103(6):1667–73. - PubMed
LinkOut - more resources
Full Text Sources