

Preconditioning donor with a combination of tacrolimus and rapamacyn to decrease ischaemia-reperfusion injury in a rat syngenic kidney transplantation model
- PMID: 22132896
- PMCID: PMC3248098
- DOI: 10.1111/j.1365-2249.2011.04487.x
Preconditioning donor with a combination of tacrolimus and rapamacyn to decrease ischaemia-reperfusion injury in a rat syngenic kidney transplantation model
Abstract
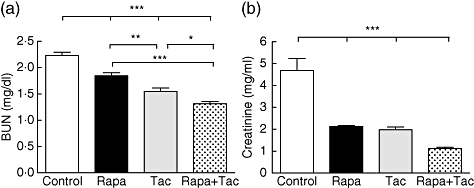
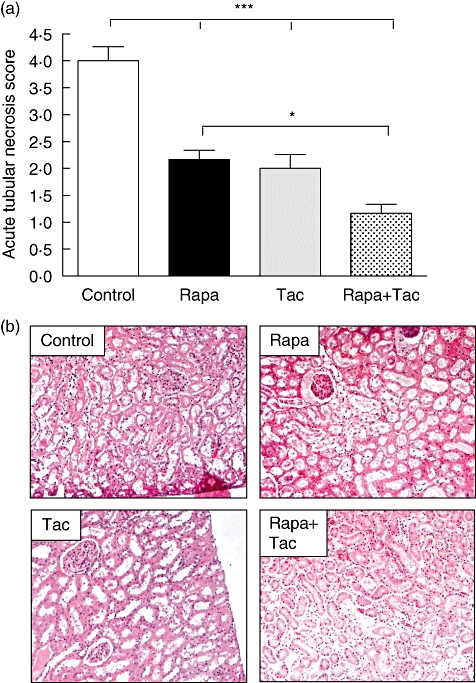
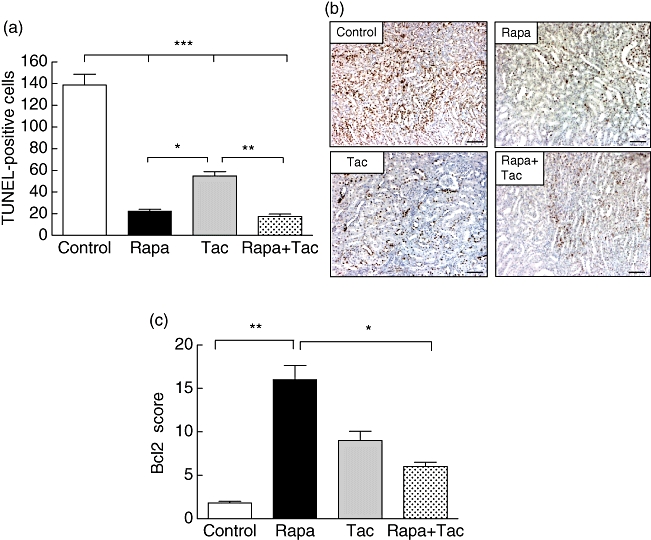
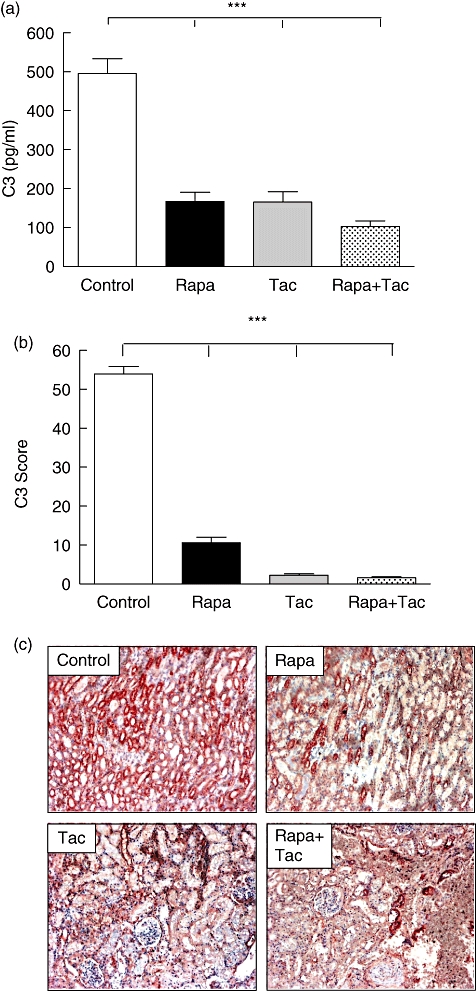
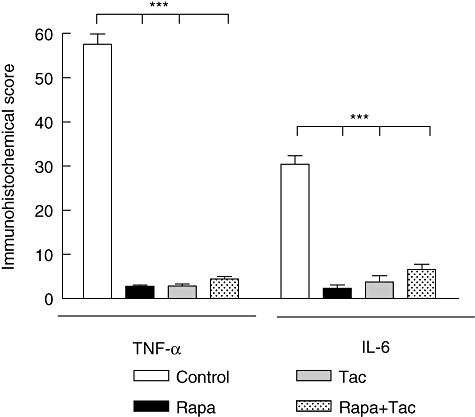
Reperfusion injury remains one of the major problems in transplantation. Repair from ischaemic acute renal failure (ARF) involves stimulation of tubular epithelial cell proliferation. The aim of this exploratory study was to evaluate the effects of preconditioning donor animals with rapamycin and tacrolimus to prevent ischaemia-reperfusion (I/R) injury. Twelve hours before nephrectomy, the donor animals received immunosuppressive drugs. The animals were divided into four groups, as follows: group 1 control: no treatment; group 2: rapamycin (2 mg/kg); group 3 FK506 (0, 3 mg/kg); and group 4: FK506 (0, 3 mg/kg) plus rapamycin (2 mg/kg). The left kidney was removed and after 3 h of cold ischaemia, the graft was transplanted. Twenty-four hours after transplant, the kidney was recovered for histological analysis and cytokine expression. Preconditioning treatment with rapamycin or tacrolimus significantly reduced blood urea nitrogen and creatinine compared with control [blood urea nitrogen (BUN): P < 0·001 versus control and creatinine: P < 0·001 versus control]. A further decrease was observed when rapamycin was combined with tacrolimus. Acute tubular necrosis was decreased significantly in donors treated with immunosuppressants compared with the control group (P < 0·001 versus control). Moreover, the number of apoptotic nuclei in the control group was higher compared with the treated groups (P < 0·001 versus control). Surprisingly, only rapamycin preconditioning treatment increased anti-apoptotic Bcl2 levels (P < 0·001). Finally, inflammatory cytokines, such as tumour necrosis factor (TNF)-α and interleukin (IL)-6, showed lower levels in the graft of those animals that had been pretreated with rapamycin or tacrolimus. This exploratory study demonstrates that preconditioning donor animals with rapamycin or tacrolimus improves clinical outcomes and reduce necrosis and apoptosis in kidney I/R injury.
© 2011 The Authors. Clinical and Experimental Immunology © 2011 British Society for Immunology.
Figures
References
-
- Tilney NL, Guttmann RD. Effects of initial ischemia/reperfusion injury on the transplanted kidney. Transplantation. 1997;64:945–7. - PubMed
-
- Shoskes DA, Halloran PF. Delayed graft function in renal transplantation: etiology, management and long-term significance. J Urol. 1996;155:1831–40. - PubMed
-
- Jang HR, Ko GJ, Wasowska BA, Rabb H. The interaction between ischemia–reperfusion and immune responses in the kidney. J Mol Med. 2009;87:859–64. - PubMed
-
- Donnahoo KK, Shames BD, Harken AH, Meldrum DR. Review article: the role of tumor necrosis factor in renal ischemia–reperfusion injury. J Urol. 1999;162:196–203. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
