

A randomized controlled evaluation of an online chronic pain self management program
- PMID: 22133450
- PMCID: PMC3514416
- DOI: 10.1016/j.pain.2011.10.025
A randomized controlled evaluation of an online chronic pain self management program
Abstract
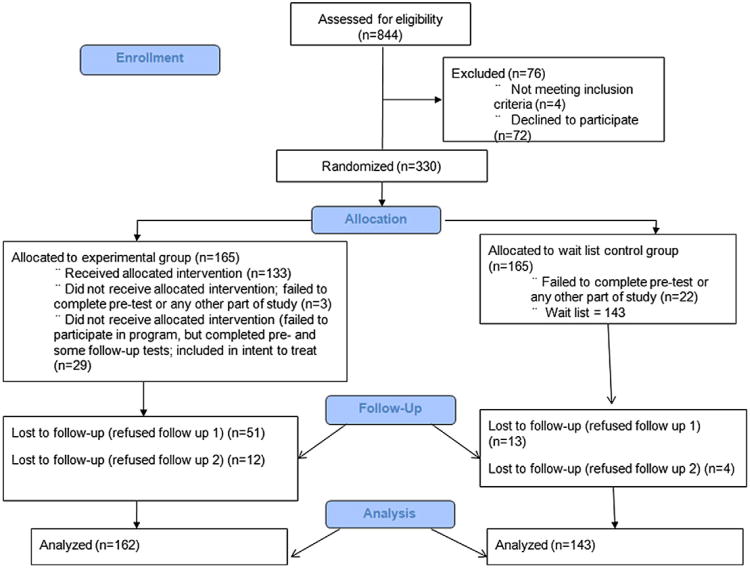
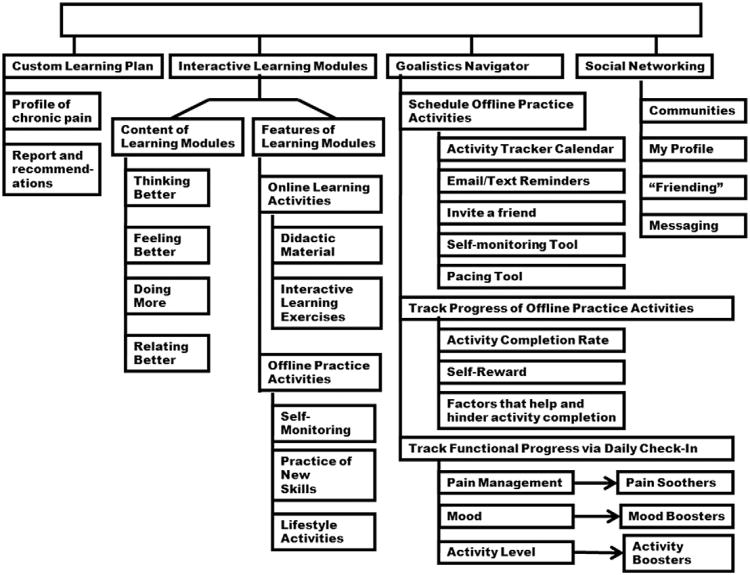
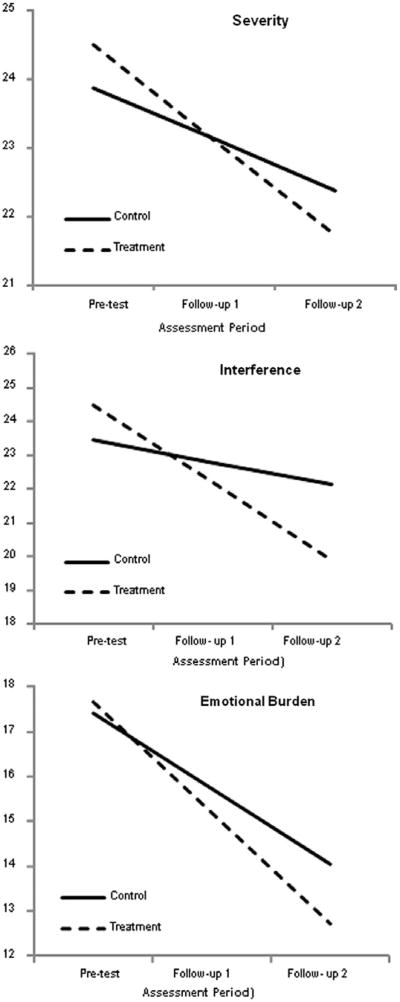
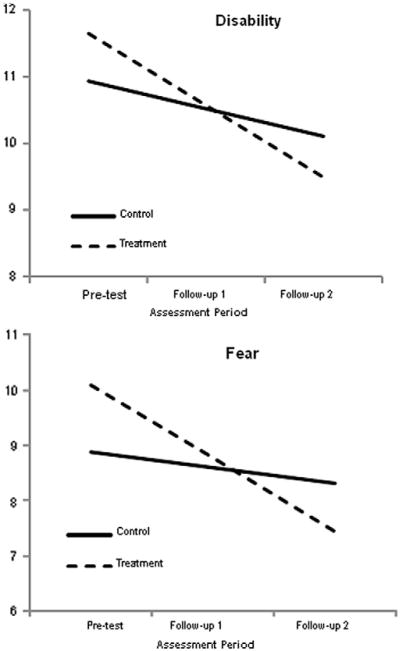
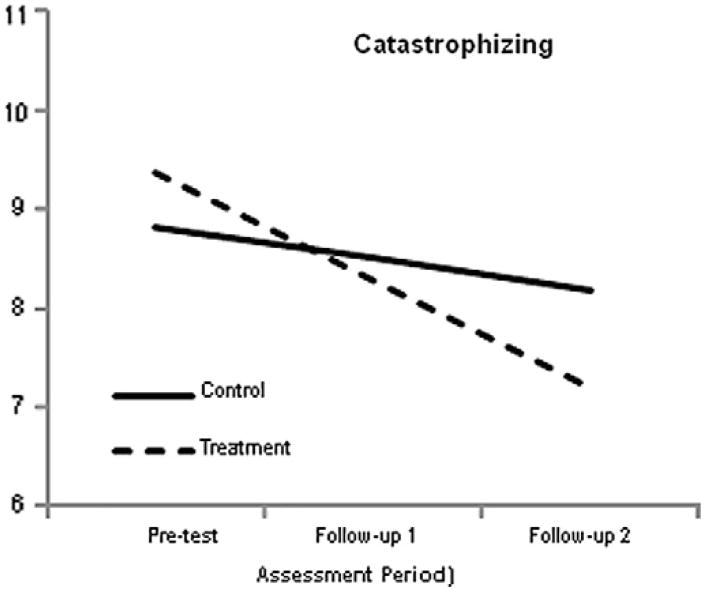
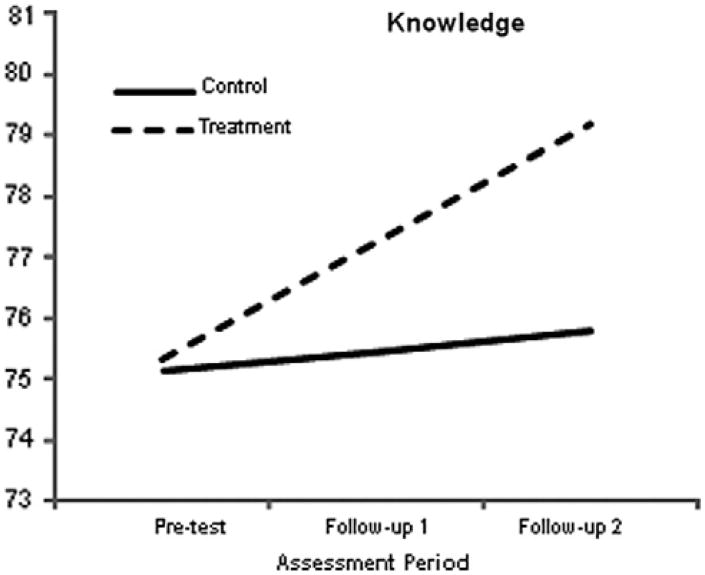
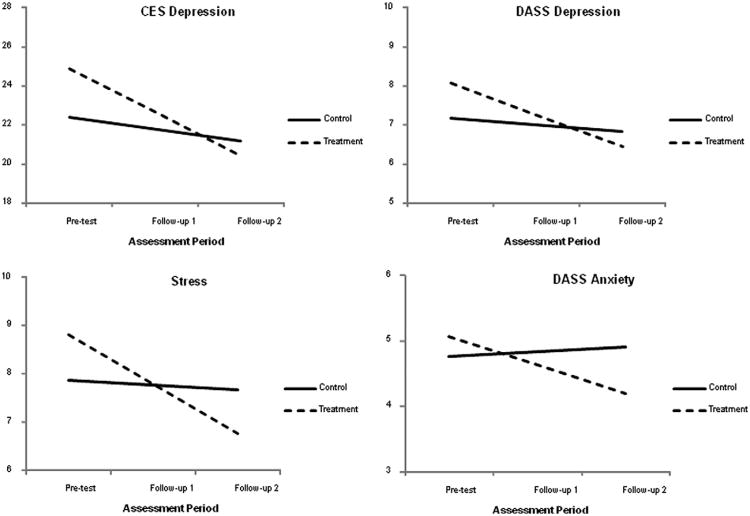
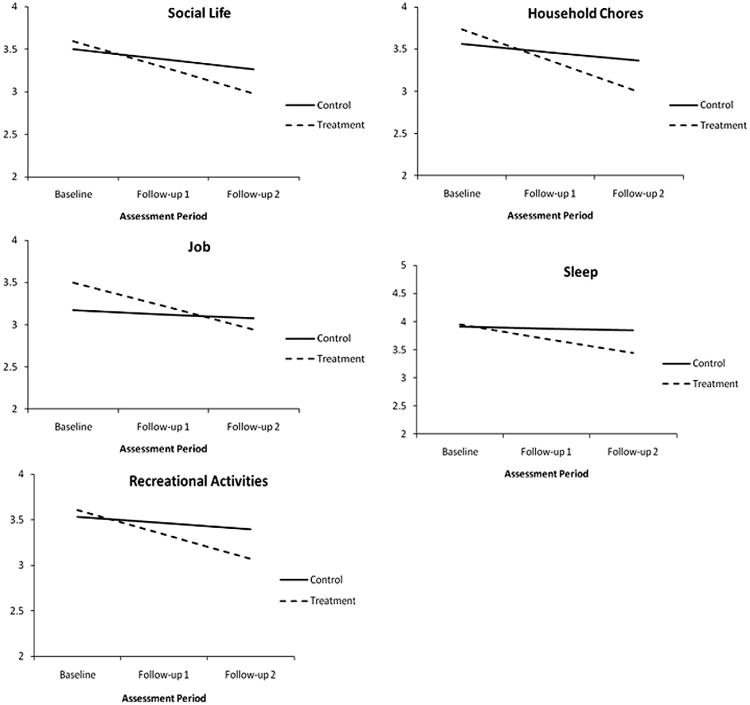
Internet-based educational and therapeutic programs (e-health applications) are becoming increasingly popular for a variety of psychological and physical disorders. We tested the efficacy of an online Chronic Pain Management Program, a comprehensive, fully self-directed and self-paced system that integrates social networking features and self-management tools into an interactive learning environment. Of 305 adult participants (196 women, 109 men), a total of 162 individuals with chronic pain were randomly assigned unsupervised access to the program for approximately 6 weeks; 143 were assigned to the wait-listed control group with treatment as usual. A comprehensive assessment was administered before the study and approximately 7 and 14 weeks thereafter. All recruitment, data collection, and participant involvement took place online. Participation was fully self-paced, permitting the evaluation of program effectiveness under real-world conditions. Intent-to-treat analysis that used linear growth models was used as the primary analytic tool. Results indicated that program utilization was associated with significant decreases in pain severity, pain-related interference and emotional burden, perceived disability, catastrophizing, and pain-induced fear. Further, program use led to significant declines in depression, anxiety, and stress. Finally, as compared to the wait-listed control group, the experimental group displayed a significant increase in knowledge about the principles of chronic pain and its management. Study limitations are considered, including the recognition that not all persons with chronic pain are necessarily good candidates for self-initiated, self-paced, interactive learning.
Copyright © 2011 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Appel PR, Bleiberg J, Noiseux J. Self-regulation training for chronic pain: can it be done effectively by telemedicine? Telemed J E Health. 2002;8:361–8. - PubMed
-
- Begg C, Cho M, Eastwood S, Horton R, Moher D, Olkin I, Pitkin R, Rennie D, Schulz KF, Simel D, Stroup DF. Improving the quality of reporting of randomized control trials. The CONSORT statement. JAMA. 1996;276:637–9. - PubMed
-
- Bender JL, Radhakrishnan A, Diorio C, Englesakis M, Jadad AR. Can pain be managed through the Internet? A systematic review of randomized controlled trials. Pain. 2011;152:1740–50. - PubMed
-
- Carlbring P, Westling BE, Ljungstrand P, Ekselius L, Andersson G. Treatment of panic disorder via the Internet: a randomized trial of a self-help program. Behav Ther. 2001;32:751–64.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
