

Review
doi: 10.1172/JCI57149.
Epub 2011 Dec 1.
The known unknowns of HPV natural history
Affiliations
- PMID: 22133884
- PMCID: PMC3225991
- DOI: 10.1172/JCI57149
Item in Clipboard
Review
The known unknowns of HPV natural history
J Clin Invest.
2011 Dec.
Abstract
The discovery that certain high-risk strains of human papillomavirus (HR-HPV) cause nearly 100% of invasive cervical cancer has spurred a revolution in cervical cancer prevention by promoting the development of viral vaccines. Although the efficacy of these vaccines has already been demonstrated, a complete understanding of viral latency and natural immunity is lacking, and solving these mysteries could help guide policies of cervical cancer screening and vaccine use. Here, we examine the epidemiological and biological understanding of the natural history of HPV infection, with an eye toward using these studies to guide the implementation of cervical cancer prevention strategies.
Figures

HPV is acquired via sexual intercourse (“incidence”), but the majority of HPV is “cleared” within 2 years in most women. Approximately 60% of women with HPV DNA detected will develop serum antibodies against HPV (HPV seropositive), and if cellular samples are collected during peak viral production, mild cytologic abnormalities may be detected on Pap smears. A minority of HPV infections persist, and individuals with persistent high-risk HPV are at a substantial risk of developing cervical precancer, or CIN3. The CIN3 lesions are the targets of screening, because more than one-third of these will progress to invasive cervical cancer within 10–20 years. The dashed lines reflect the uncertainty in the natural history of HPV. Namely, it is unclear whether anti-HPV antibody developed following natural HPV infection protects against reinfection, and whether loss of HPV detection reflects virologic clearance or establishment of viral latency.

State a: sexually inexperienced, HPV uninfected; state b: HPV infected, HPV DNA positive; state c: HPV DNA negative; state c1: HPV uninfected, immune; state c2: HPV uninfected, susceptible; state c3: HPV infected, HPV DNA negative, immune; state d: new or recurrent HPV DNA positive. See text for further explanation.

All women in the analysis were DNA negative for the relevant vaccine HPV type at baseline. Blue, rate of new DNA detection among women HPV seronegative for the same HPV type; red, rate of new DNA detection among women HPV seropositive for the same HPV type. Adapted with permission from Sexually Transmitted Diseases (48).
Reprinted with permission from Vaccine (23).
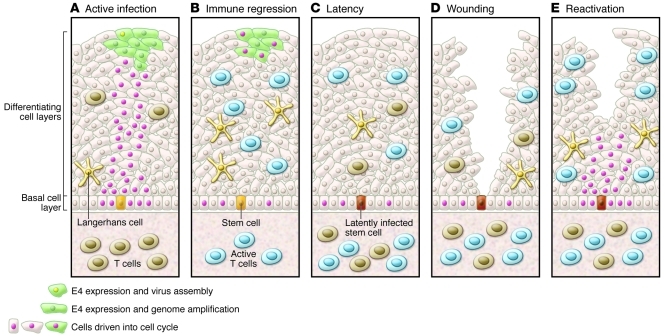
(A) Active infection drives cells in the basal layer and above into cell cycle, allowing genome amplification and new virion production. (B) Triggering of an effective immune response leads to immune regression, accompanied by infiltration of predominantly T cells. (C) Viral latency may ensue, with viral genomes restricted to stem cells in the basal layer of the epithelium. (D and E) Wounding may stimulate latently infected basal cells to divide and trigger reactivation and stimulation of tissue-resident memory T cells. Adapted with permission from Virology (63).
References
-
- Munoz N, et al. Impact of human papillomavirus (HPV)-6/11/16/18 vaccine on all HPV-associated genital diseases in young women. J Natl Cancer Inst. 2010;102(5):325–339. - PubMed
