

Critical role of activated protein C in early coagulopathy and later organ failure, infection and death in trauma patients
- PMID: 22133894
- PMCID: PMC3549308
- DOI: 10.1097/SLA.0b013e318235d9e6
Critical role of activated protein C in early coagulopathy and later organ failure, infection and death in trauma patients
Abstract
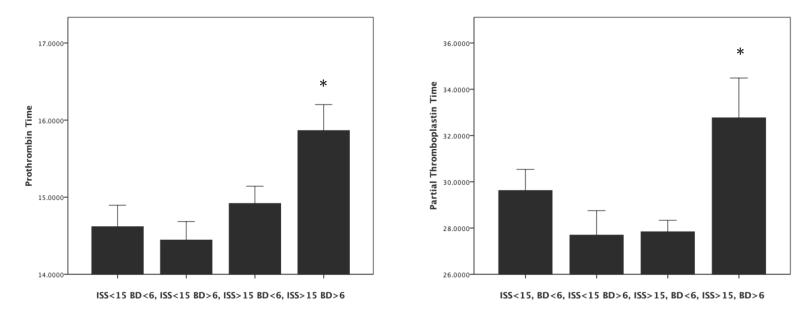
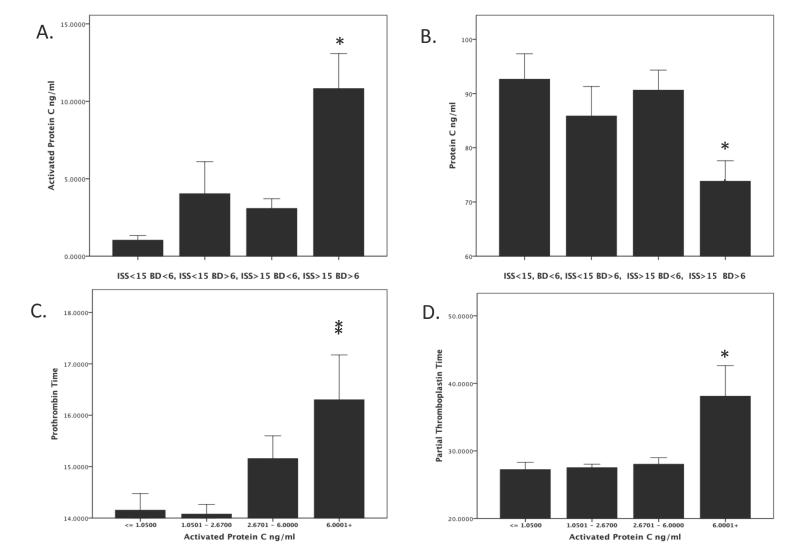
Background: Recent studies have identified an acute traumatic coagulopathy that is present on admission to the hospital and is independent of iatrogenic causes. We have previously reported that this coagulopathy is due to the association of severe injury and shock and is characterized by a decrease in plasma protein C (PC) levels. Whether this early coagulopathy and later propensity to infection, multiple organ failure and mortality are associated with the activation of PC pathway has not been demonstrated and constitutes the aim of this study.
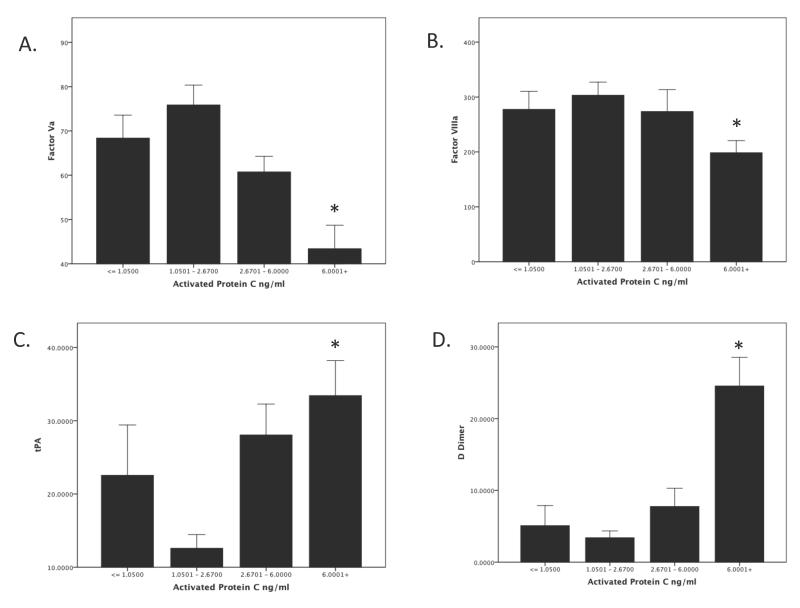
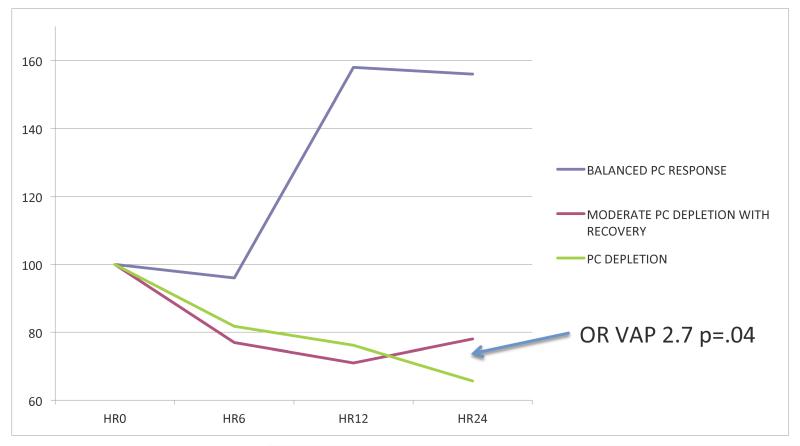
Methods and findings: This was a prospective cohort study of 203 major trauma patients. Serial blood samples were drawn on arrival in the emergency department, and at 6, 12, and 24 hours after admission to the hospital. PT, PTT, Va, VIIIa, PC aPC t-PA, and D-dimer levels were assayed. Comprehensive injury, resuscitation, and outcome data were prospectively collected. A total of 203 patients were enrolled. Patients with tissue hypoperfusion and severe traumatic injury showed a strong activation of the PC which was associated with a coagulopathy characterized by inactivation of the coagulation factors V and VIII and a derepression of the fibrinolysis with high plasma levels of plasminogen activator and high D-dimers. Elevated plasma levels of activated PC were significantly associated with increased mortality, organ injury, increased blood transfusion requirements, and reduced ICU ventilator-free days. Finally early depletion of PC after trauma is associated with a propensity to posttraumatic ventilator-associated pneumonia.
Conclusions: Acute traumatic coagulopathy occurs in the presence of tissue hypoperfusion and severe traumatic injury and is mediated by activation of the PC pathway. Higher plasma levels of aPC upon admission are predictive of poor clinical outcomes after major trauma. After activation, patients who fail to recover physiologic plasma values of PC have an increased propensity to later nosocomial lung infection.
Figures
References
-
- Injury Chart Book. World Health Orginization; Geneva:
-
- Holcomb JB, Jenkins D, Rhee P, Johannigman J, Mahoney P, Mehta S, Cox ED, Gehrke MJ, Beilman GJ, Schreiber M, et al. Damage control resuscitation: directly addressing the early coagulopathy of trauma. The Journal of trauma. 2007;62(2):307–310. - PubMed
-
- Hess JR, Holcomb JB, Hoyt DB. Damage control resuscitation: the need for specific blood products to treat the coagulopathy of trauma. Transfusion. 2006;46(5):685–686. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
