

Renal phosphate loss in long-term kidney transplantation
- PMID: 22134626
- PMCID: PMC3280026
- DOI: 10.2215/CJN.06380611
Renal phosphate loss in long-term kidney transplantation
Abstract
Background and objectives: Renal phosphate wasting occurs early postkidney transplantation as a result of an accumulation of parathyroid hormone and fibroblast growth factor 23 from the CKD period. Serum phosphate, parathyroid hormone, and fibroblast growth factor 23 return to baseline 1 year postkidney transplantation. What happens beyond this period is unknown.
Design, setting, participants, & measurements: Mineral parameters were obtained from 229 kidney transplant recipients at least 1 year posttransplantation; 46 normal subjects and 202 CKD patients with similar GFR served as controls. Factors associated with phosphate metabolism were analyzed.
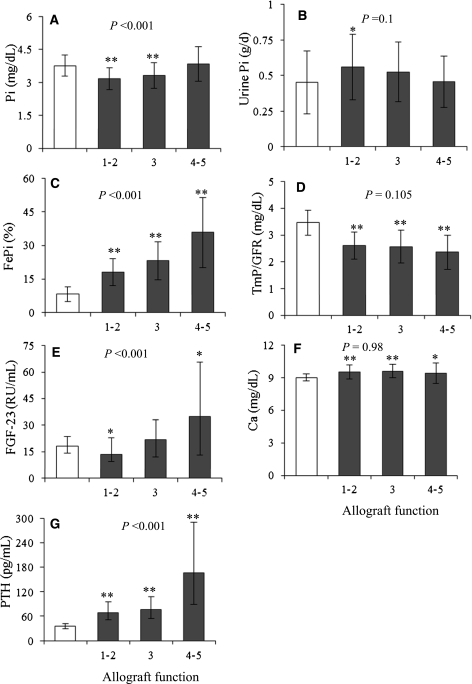
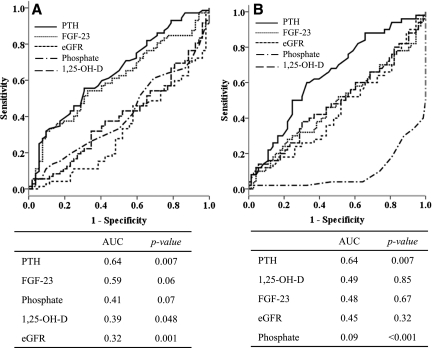
Results: Despite the reduced graft function, most kidney transplant recipients had lower serum phosphate than normal subjects accompanied by renal phosphate loss. Fibroblast growth factor 23 was mostly lower or comparable with normal subjects, whereas parathyroid hormone was elevated in most patients. Hyperparathyroidism is also more common among kidney transplant recipients compared with CKD patients. Both parathyroid hormone and fibroblast growth factor 23 showed relationships with renal phosphate excretion, but only parathyroid hormone displayed an independent association. Parathyroid hormone showed the highest area under the curve in predicting renal phosphate leak. When patients were categorized according to parathyroid hormone and fibroblast growth factor 23 levels, only subset of patients with high parathyroid hormone had an increased renal phosphate excretion.
Conclusions: Relatively low serum phosphate from renal phosphate leak continued to present in long-term kidney transplantation. Both parathyroid hormone and fibroblast growth factor 23 participated in renal tubular phosphate handling, but persistent hyperparathyroidism seemed to have a greater influence in this setting.
Figures

Similar articles
-
Hyperparathyroidism and increased fractional excretion of phosphate predict allograft loss in long-term kidney transplant recipients.Clin Exp Nephrol. 2017 Oct;21(5):926-931. doi: 10.1007/s10157-016-1370-9. Epub 2016 Dec 16. Clin Exp Nephrol. 2017. PMID: 27981393
-
Dialysis vintage and parathyroid hormone level, not fibroblast growth factor-23, determines chronic-phase phosphate wasting after renal transplantation.Bone. 2012 Oct;51(4):729-36. doi: 10.1016/j.bone.2012.06.027. Epub 2012 Jul 14. Bone. 2012. PMID: 22796419
-
Serum level of fibroblast growth factor 23 in maintenance renal transplant patients.Nephrol Dial Transplant. 2012 Nov;27(11):4227-35. doi: 10.1093/ndt/gfs409. Nephrol Dial Transplant. 2012. PMID: 23144073
-
Fibroblast growth factor 23 in chronic kidney disease: New insights and clinical implications.Nephrology (Carlton). 2011 Mar;16(3):261-8. doi: 10.1111/j.1440-1797.2011.01443.x. Nephrology (Carlton). 2011. PMID: 21265930 Review.
-
Phosphate and FGF-23 homeostasis after kidney transplantation.Nat Rev Nephrol. 2015 Nov;11(11):656-66. doi: 10.1038/nrneph.2015.153. Epub 2015 Sep 29. Nat Rev Nephrol. 2015. PMID: 26416497 Review.
Cited by
-
Hyperparathyroidism and increased fractional excretion of phosphate predict allograft loss in long-term kidney transplant recipients.Clin Exp Nephrol. 2017 Oct;21(5):926-931. doi: 10.1007/s10157-016-1370-9. Epub 2016 Dec 16. Clin Exp Nephrol. 2017. PMID: 27981393
-
Long-term clinical practice experience with cinacalcet for treatment of hypercalcemic hyperparathyroidism after kidney transplantation.Biomed Res Int. 2015;2015:292654. doi: 10.1155/2015/292654. Epub 2015 Mar 10. Biomed Res Int. 2015. PMID: 25861621 Free PMC article.
-
Optimization of Bone Health in Children before and after Renal Transplantation: Current Perspectives and Future Directions.Front Pediatr. 2014 Feb 24;2:13. doi: 10.3389/fped.2014.00013. eCollection 2014. Front Pediatr. 2014. PMID: 24605319 Free PMC article. Review.
-
Changes in clinical indicators related to the transition from dialysis to kidney transplantation-data from the ERA-EDTA Registry.Clin Kidney J. 2019 Jul 1;13(2):188-198. doi: 10.1093/ckj/sfz062. eCollection 2020 Apr. Clin Kidney J. 2019. PMID: 32296524 Free PMC article.
-
FGF23 in kidney transplant: the strange case of Doctor Jekyll and Mister Hyde.Clin Kidney J. 2016 Oct;9(5):665-8. doi: 10.1093/ckj/sfw072. Epub 2016 Sep 6. Clin Kidney J. 2016. PMID: 27679712 Free PMC article.
References
-
- Gutierrez O, Isakova T, Rhee E, Shah A, Holmes J, Collerone G, Juppner H, Wolf M: Fibroblast growth factor-23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J Am Soc Nephrol 16: 2205–2215, 2005 - PubMed
-
- Imanishi Y, Inaba M, Nakatsuka K, Nagasue K, Okuno S, Yoshihara A, Miura M, Miyauchi A, Kobayashi K, Miki T, Shoji T, Ishimura E, Nishizawa Y: FGF-23 in patients with end-stage renal disease on hemodialysis. Kidney Int 65: 1943–1946, 2004 - PubMed
-
- Claesson K, Hellman P, Frodin L, Rastad J: Prospective study of calcium homeostasis after renal transplantation. World J Surg 22: 635–641, 1998 - PubMed
-
- Bhan I, Shah A, Holmes J, Isakova T, Gutierrez O, Burnett SM, Juppner H, Wolf M: Post-transplant hypophosphatemia: Tertiary 'hyper-phosphatoninism'? Kidney Int 70: 1486–1494, 2006 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
