

Computed Tomography (CT) Imaging of Injuries from Blunt Abdominal Trauma: A Pictorial Essay
- PMID: 22135535
- PMCID: PMC3216157
Computed Tomography (CT) Imaging of Injuries from Blunt Abdominal Trauma: A Pictorial Essay
Abstract
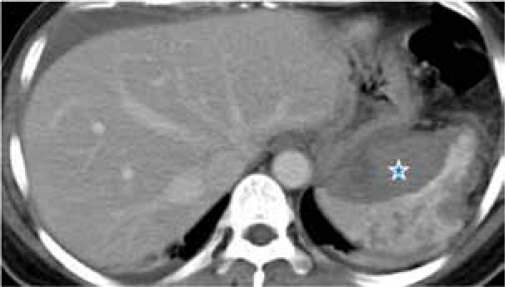
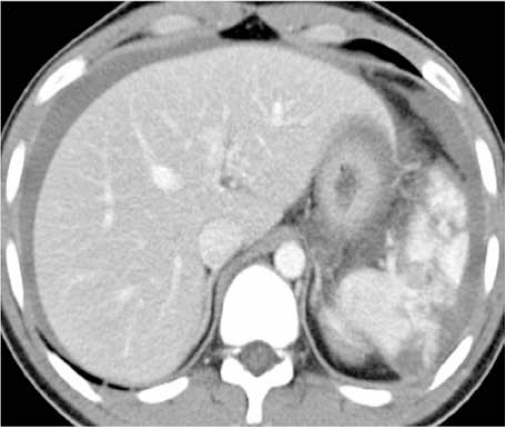
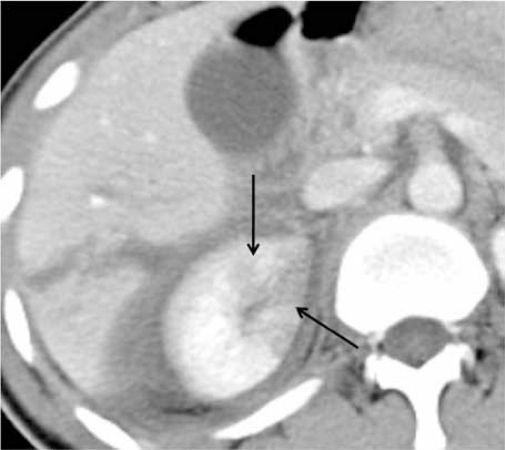
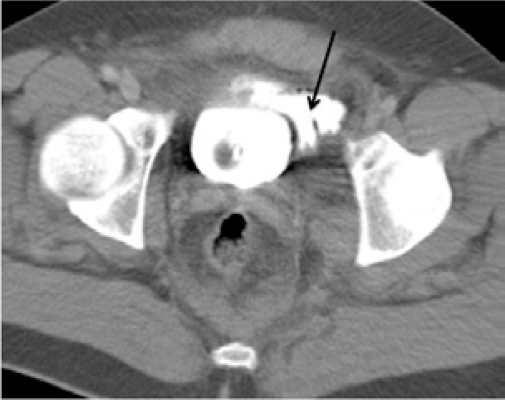
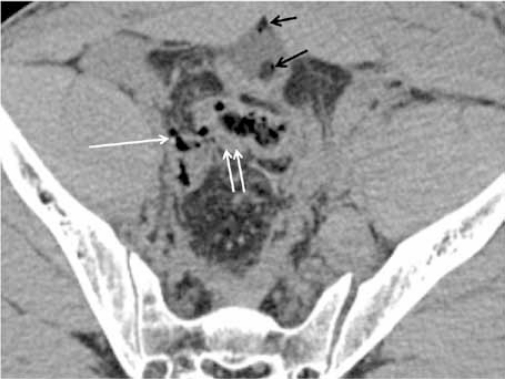
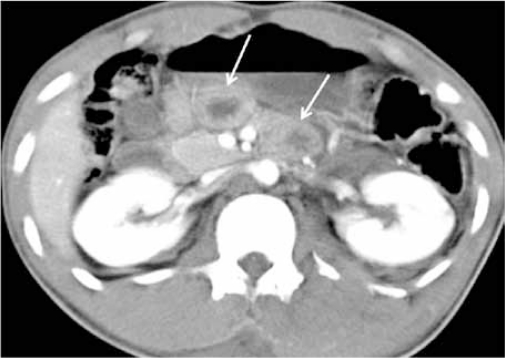
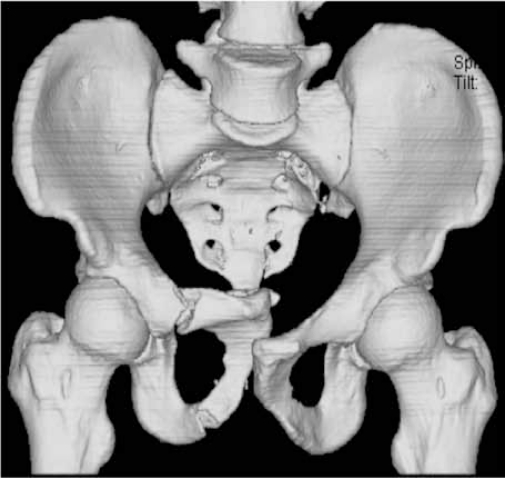
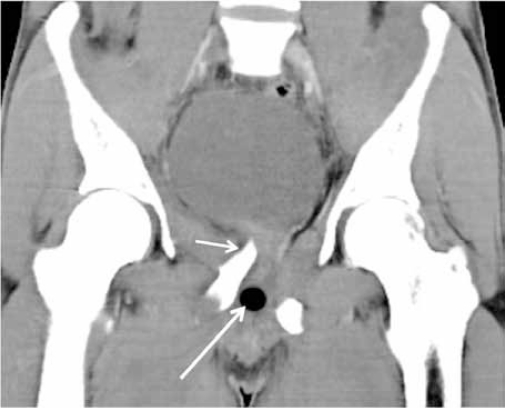
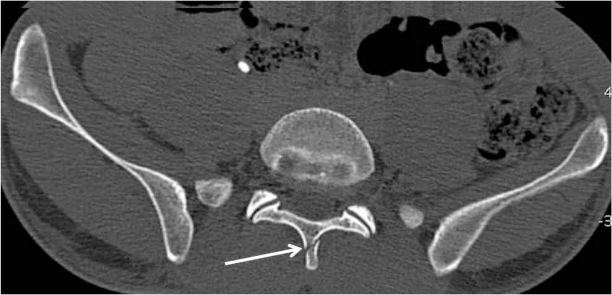
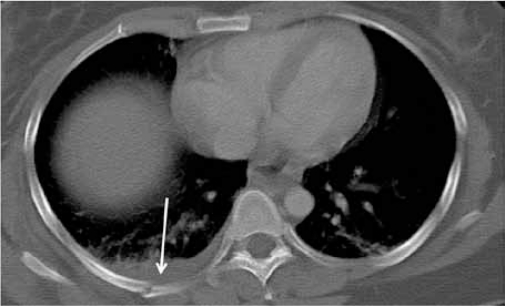
Blunt abdominal trauma can cause multiple internal injuries. However, these injuries are often difficult to accurately evaluate, particularly in the presence of more obvious external injuries. Computed tomography (CT) imaging is currently used to assess clinically stable patients with blunt abdominal trauma. CT can provide a rapid and accurate appraisal of the abdominal viscera, retroperitoneum and abdominal wall, as well as a limited assessment of the lower thoracic region and bony pelvis. This paper presents examples of various injuries in trauma patients depicted in abdominal CT images. We hope these images provide a resource for radiologists, surgeons and medical officers, as well as a learning tool for medical students.
Keywords: blunt abdominal trauma; computed tomography; injuries; medical sciences.
Figures














References
-
- Federle MP, Goldberg HI, Kaiser JA, Moss AA, Jeffrey RB, Mail JC. Evaluation of abdominal trauma by computed tomography. Radiology. 1981;138:637–644. - PubMed
-
- Shuman WP. CT of blunt abdominal trauma. Radiology. 1997;205:297–306. - PubMed
-
- Rhea JT. The frequency and significance of thoracic injuries detected on abdominal CT scans of multiple trauma patients. J Trauma. 1989;29(4):502–505. - PubMed
-
- Hoff WS, Holevar M, Nagy KK, Patterson L, Young JS, Arrillaga A, et al. Practice management guidelines for the evaluation of blunt abdominal trauma: the EAST practice management guidelines work group. J Trauma. 2002;53:602–615. - PubMed
-
- Ferrada R, Rivera D, Ferrada P. In: Blunt Abdominal Trauma. General Surgery. 2nd ed. Bland KI, Sarr MG, Buchler MW, Csendes A, et al., editors. London: Springer; 2009. pp. 87–96.
LinkOut - more resources
Full Text Sources